

Division
East Florida
Hospital
HCA Florida Northwest Hospital
Specialty
Internal Medicine
Document Type
Poster
Publication Date
2023
Keywords
pleural effusion, rib fracture, fall, aged
Disciplines
Internal Medicine | Medicine and Health Sciences | Respiratory Tract Diseases
Abstract
INTRODUCTION Delayed pleural effusion (DPL) post rib fracture is a lesser known and not adequately studied entity. DPL is associated with increased hospital/ICU length of stay (LOS) and poorer disposition at discharge. Some case series have reported incidence as high as 40.8 % making it a clinically significant complication to watch for.
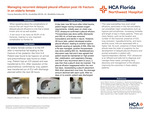
CASE An elderly female presented to the ED after a mechanical fall leading to right side fractured ribs (5th to 9th rib posteriorly) and pneumothorax. Patient was hypoxic in ER and an ICD was placed. Trauma series showed right pulmonary contusion but no hemothorax or any other injury. There was complete resolution of pneumothorax in ICU and ICD was removed. Post ICD removal repeat X-ray was negative for any pneumothorax and patient was moved out of ICU with plan to discharge in next 24- 48hrs. The patient started having increasing oxygen requirement the next day, ie 96 hrs after trauma. Chest x-ray and POC ultrasound confirmed suspicion of pleural effusion. Thoracentesis was done and 350 ml of fluid was removed with remarkable improvement in patient’s condition. The pleural fluid was transudative and sterile. Over the next 48hrs the pleural effusion recollected leading to hypoxia induced atrial fibrillation. It was managed with a diltiazem drip and amiodarone . After multidisciplinary discussion about management options, it was decided that we will go ahead with a thoracentesis one more time and if fluid reaccumulates, we will proceed with pleurX drain placement . The patient was deemed too frail for pleurodesis. This time, 650 ml was drained on thoracentesis of the same type as before. Supportive management with high protein diet, mobilization and respiratory therapy continued. The pleural effusion reappeared over the next 48 hrs necessitating pleurX placement. It was drained every 48-72 hours depending on the patients condition. The drained amount declined with each cycle and the interval was gradually increased. Afterwards, patient was discharged after 2 weeks in hospital
DISCUSSION Many processes contribute to fluid accumulation post rib fractures. A disruption in the pressure seal by trauma (i.e. rib fracture and pulmonary contusion) as well as increased local pro-inflammatory response favors pleural accumulation. Hypoalbuminemia also contributes to pleural effusion by decreasing oncotic pressure. This case exemplifies how small pleural effusions in the frail and elderly can precipitate hypoxia and arrhythmia leading to hemodynamic compromise, increasing morbidity and LOS. All pleural fluid cultures were negative in our patient so the patient’s deterioration was likely due to the effusion and not possible infection. The patient’s LOS likely would not have been more than 96 hours if it was not complicated by DPL. The location and number of rib fractures, presence of ICD, lung contusion, hypoalbuminemia, and injury severity score have been associated with higher risk of developing DPL. In these higher risk patients, POC ultrasound is an efficient and safe method to swiftly be able to diagnose these effusions when the suspicion is high. Early diagnosis and aggressive management of these DPLs are crucial to improving outcomes in the elderly.
Recommended Citation
Ramadan, Yaseen; Swatisikta, Fnu; and Golawala, Mushfeka Baker, "Managing Recurrent Delayed Pleural Effusion Post Rib Fracture in an Elderly Female" (2023). East Florida Division GME Research Day 2023. 2.
https://scholarlycommons.hcahealthcare.com/eastflorida2023/2