


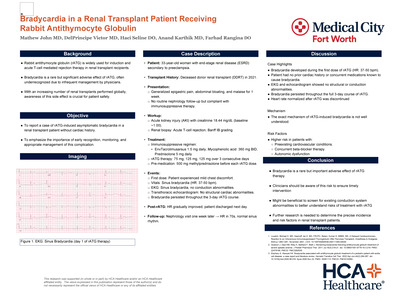
North Texas Research Forum 2025
On April 18, 2025, Medical City Arlington hosted the North Texas Division Research Forum with 200+ attendees (in-person & virtual), over 350 authors, 12 oral presentations, 46 in-person poster presentations, and 50 virtual poster presentations celebrating scholarly activity from the North Texas Regional Consortium of Medical City Healthcare, University of North Texas (UNT), and Texas Christian University (TCU). The forum was honored to have Dr. Kimberly Washington, MD, FACS - Assistant Professor, Department of Surgery, Assistant Dean of Clinical Faculty Success & Engagement, TCU and Hepato-Pancreato-Biliary Surgery, Texas Health Physician Group as the keynote speaker focusing on “Patient Experience: Oncologic Surgery”.
Research Category Winners
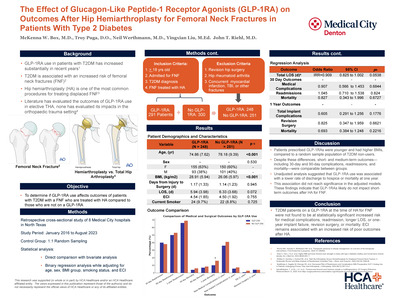
- 1st Place: McKenna Box, Neil Werthmann, Troy Puga, Andrew Jen, Yingxian Liu, and John Riehl - A Retrospective Cross-Sectional Study of GLP-1 Agonist Effects on Outcomes after Total Knee Arthroplasty
- 2nd Place: Luke Taylor, Otoniel Espinoza, Omar O. Hernandez, Shannon Biggers, Shirin Miller, Srinivas Yallapragada, Amer Alaiti, Andrew Fredericks, Song Li, and Claudius Mahr - Use of VA ECMO in Patients with Acute Pulmonary Embolism Presenting with Obstructive Cardiogenic Shock undergoing Mechanical Thrombectomy
- 3rd Place: Troy Puga, Tanner Haechten, Cole Cush, Hans Drawbert, and John Riehl - NFL Kick-off Rule Change: A Comparative Analysis of Injury Incidence
Quality Improvement Category Winners
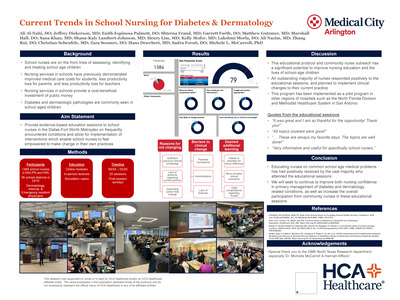
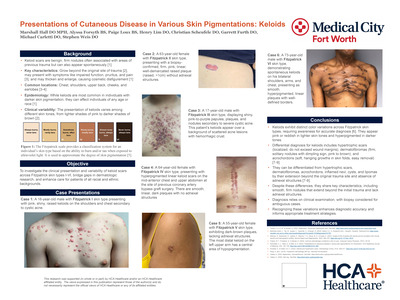
- 1st Place: Matthew Gutzmer, Michele L. McCarroll, Christian Scheufele, Zara Soomro, Ali Nazim, Enith Espinosa-Palmett, Marshall Hall, Taylor Pickering, Garrett Furth, Jasmine Silva, Shterna Frand, Shana Lambert-Johnson, Jeff Dickerson, Henry Lim, Ali Al-Nahi, Kelly Mofor, Lakshmi Morla, Nischal Pokhrel, Brina Gonzalez, Rui Zhang, Sana N Khan, Devika Adusumilli, and Sherri Morgan - Improving Nursing Professional Practice-Based Application Using the Latest Evidence-Based Approaches in Dermatology and Diabetes
- 2nd Place: Makenzie Morrissey, Kristen Payne, Randall Rittmann, Chris Robert, Joseph Lim, and Danielle Pigneri - Improving Communication and Follow Up for Incidental Findings from PanScan Imaging
- 3rd Place: Sumanth Reddy, Artur Amirkhanyan, Jeremiah Avarana, Praneetha Arge, and Alicia Lay - Effective Communication in the Pronunciation of Brain Death
Case Report Category Winners
- 1st Place: Dakota Dalton, Elizabeth White, and Christopher Medina - Efficacy of Osteopathic Manipulative Treatment in Post-Stroke Recovery Patients
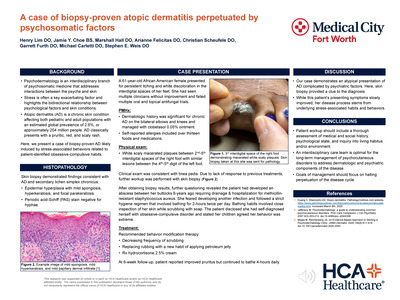
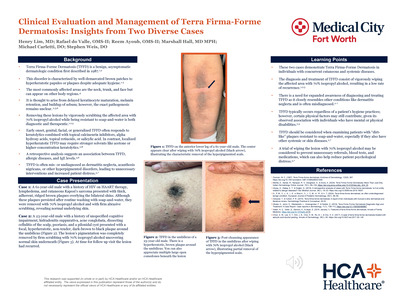
- 2nd Place: Rafael Do Valle, Reem Ayoub, Henry Lim, Marshall Hall, and Stephen Weis - Clinical Evaluation and Management of Terra Firma-Forme Dermatosis: Insights from Two Diverse Cases
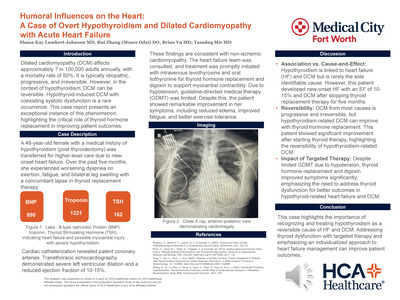
- 3rd Place: Shana-Kay Lambert-Johnson, Rui Zhang, Brian Yu, and Tasaduq Mir - Humoral Influences on the Heart: A Case of Overt Hypothyroidism and Dilated Cardiomyopathy with Acute Heart Failure
Posters and presentations are also available at the North Texas Division GME Research Forum Gallery here.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-

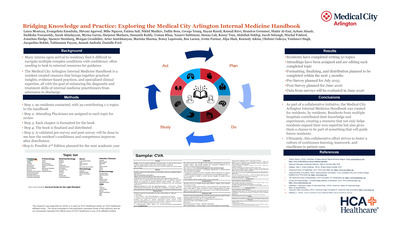
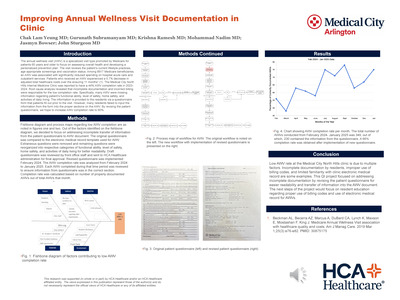
The “OB Guide”: A Proposed Adjunct to the “Intern Survival Guide” and its Effect on Resident Wellness
Aaishah Vohra, Lola Adeleye, Zara Soomro, Maria Crompton, and Tasaduq Mir
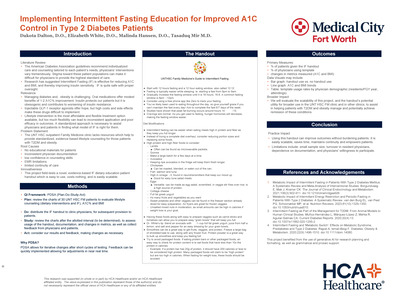
Background: Residency is defined by constant change. The expectations, specialty, preceptor teaching styles and varied knowledge sets needed for each rotation differ greatly. As a result, residents are forced to adapt their learning styles quickly, to ensure they optimize the small amount of time allotted to them. Multiple studies have shown the high levels of stress, depression, anxiety and impostor syndrome that run rampant throughout medical learners, residents included. Our residency program has recently started a new obstetrics rotation with many requirements still unknown. This study evaluates the efficacy of the update to the “The Intern Survival Handbook” in mitigating stressors among new trainees, enhancing their work performance, and promoting overall mental health, specifically with a new obstetrics and gynecology rotation. Methods: We have created a short, easily digestible “chapter” to the “Intern Survival Guide” with information provided to us by Medical City Arlington OB Residents. The knowledge that they have imparted includes shift hours, important personnel (residents and attendings), workflow, note templates, presentation guidelines, and common assessment workups. We plan to administer 2 surveys. One in February 2025 evaluating the desire for an update and one in May 2025 evaluating the effect of the chapter on overall resident wellness. Results The results will depend on the final survey, which will be completed in March 2025 Discussion We hope that with the implementation of an “OB Guide" as an adjunct to the “Intern Survival Guide” to decrease the stress of unknown rotation parameters among fellow residents in addition to improving workflow, and increasing overall resident wellness.
-

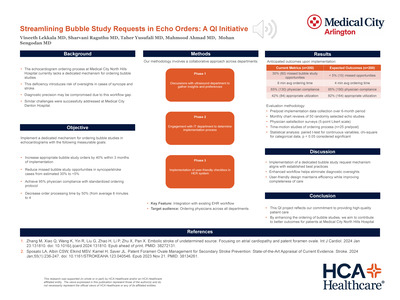
There’s a QR Code For That: Trauma Performance Improvement, Patient Safety, and Peer Review
April Miller, Luis Taveras, Elizabeth Kim, and Kathy Galt
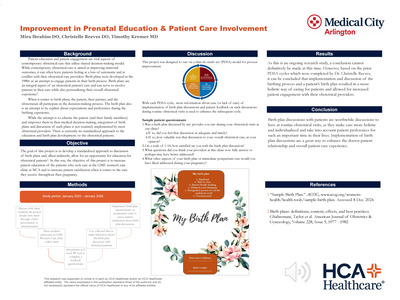
In preparation for our facility’s initial ACS verification visit, a Trauma Consultative Site visit in 2021 identified the need for a streamlined process to communicate issues to the Trauma Program that were recognized during patient care. This was especially true on weekends and nights when issues were most likely to occur. A recent literature review revealed implementation of electronic communication tools increased reporting of performance improvement and patient safety (PIPS) events and improved tracking and resolution of events. The authors of that study used a virtual chatroom accessible from cell phone to post PIPS events. One perceived drawback to this method is that reporting cannot be done anonymously if so desired.1 We sought to improve reporting in our facility by providing a rapid, easily accessible, user-friendly, and potentially anonymous method of reporting that any staff member could access. A reporting platform was created to input information regarding PIPS concerns. A QR code was designed which allows providers and staff to input information into a HIPAA compliant access point site, hosted in a Microsoft Forms platform. The report can be made anonymously. The share point site is then accessible by the Trauma Services department to capture all these PIPS issues. The access point notifies the trauma coordinators and the Trauma Program director in real time and the issues are processed within our Trauma PIPS Review Policy. Once addressed, the PI issue is then archived. Information collected includes patient name (if applicable), type and details of the issue, unit of the hospital where occurring, and reporter’s name (not required). Of note, this product is a patient safety work product document. It is protected from disclosure pursuant to the provisions of the Patient Safety and Quality Improvement Act (42 CFR Part 3) and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited. A QR code-based reporting system is an accessible and easy to use platform for PIPS reporting, additionally with the benefit of anonymity if needed. A more efficient process can result in increased reporting and optimization of the process to identify and rectify issues. Since implementation of the QR code in March 2022, we have been able to measure the effects of the change by examining the number of PIPS issues submitted each month. On average, fourteen reports have been received each month, with the most commonly reporting departments being the trauma surgeons and the emergency department. The change was implemented and continues to be sustained by distributing flyers in the work areas of trauma staff including, but not limited to: call rooms, the OR lounge, emergency department, radiology, surgical units, and ICU. Given the positive response from the staff and the improved PIPS reporting, this hospital system is now offering the application to all other trauma programs, with launch recently at a Level 1 trauma/burn facility. As the process rolls out in other hospitals, we intend to continue to evaluate the effect with pre-and post-rollout monitoring.
-

Todd's Paralysis: Sharpnel-Induce Seizure
Kenny Tran and Alain Folefack
When evaluating seizure in war veterans, distinguishing new-onset hemiparesis with aphasia from stroke can be challenging due to prior brain injury and anticonvulsant therapy. This case involves a patient with a shrapnel injury displaying stroke-symptoms after a seizure highlights the differences between stroke and seizure-related deficits in this population. Careful consideration of imaging, history and clinical presentation are essential for accurate diagnosis and management.
-

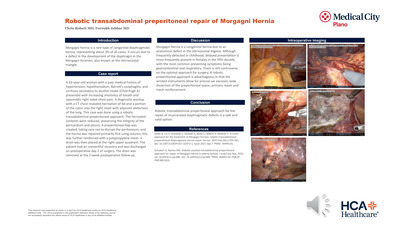
Traumatic Rupture of Gall Bladder After Blunt Trauma
Chris Robert and Alicia Lay
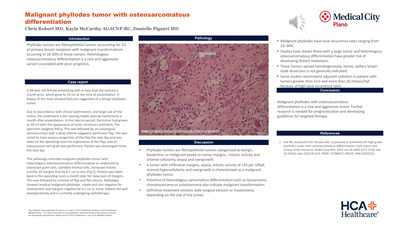
Introduction: Gallbladder injury accounts for less than 1% of the patient presenting with blunt abdominal trauma, due to its protected location in the undersurface of the liver. Case report: A 41-year-old male presented to the emergency department after a motor vehicle collision. Patient was hemodynamically stable; on exam, patient had focal tenderness in the lower abdomen. Initial lab results revealed elevated blood alcohol of 302 mg/dl, elevated lactate of 3.9 mmol/l, a white blood cell count of 6.76 K/mm3, and a hemoglobin of 15.2 g/dl. Patient was pan-scanned as per trauma protocol. A computed tomography scan revealed a mesenteric hematoma associated with the hepatic flexure of the colon and mural thickening suspicious for colonic serosal injury. A small amount of intraperitoneal fluid more evident in the perihepatic and perisplenic regions was seen without free air. The other associated injury was a right temporomandibular joint subluxation. Patient was initially managed with serial abdominal exams and hemoglobin trends but continued to have persistent abdominal pain with nausea and tachycardia. In view of worsening symptoms, the patient was taken up for a diagnostic laparoscopy on day 2 of presentation. Upon entry, a blood clot was visualized overlying the omentum, when rotated away from this region, revealed bile-stained bowel. At this point, we converted it to an open laparotomy. We dissected the omentum from the transverse colon and entered the lesser sac, further dissecting along the right lateral white line of Toldt to expose the ascending and transverse colon at the hepatic flexure, which revealed a perforated gall bladder. We performed a cholecystectomy in retrograde fashion after the cystic artery, accessory cystic artery, and cystic duct were identified and ligated. Pathology revealed a 1.5 cm defect in the fundus of the gall bladder. Patient did well postoperatively and was discharged on postoperative Day 4. Learning points: Gall bladder injuries from blunt abdominal trauma are rare due to its protected position embedded in the undersurface of the liver. Motor vehicle collision is the most common cause of blunt gallbladder injury. A thin gallbladder wall, distended gallbladder, and recent alcohol ingestion can predispose to gall bladder injury. Isolated gall bladder perforations are rare, and they are commonly associated with injuries of the liver, small bowel, spleen, kidney, pancreas, or abdominal vascular injury. They are challenging to diagnose due to vague symptoms of pain, and patients generally do not appear toxic on presentation. They present either during damage control surgery incidentally or with non-specific abdominal pain a few days after trauma. Conclusion: A gall bladder injury can be difficult to diagnose because of vague symptoms, and a high index of suspicion is required. Once diagnosed, an open or laparoscopic cholecystectomy is the definitive management.
-

Treatment of Starvation Ketoacidosis in the Third Trimester of Pregnancy: A Case Report
Christine Le, Charmaine Oladell, and Nicole Tenzel
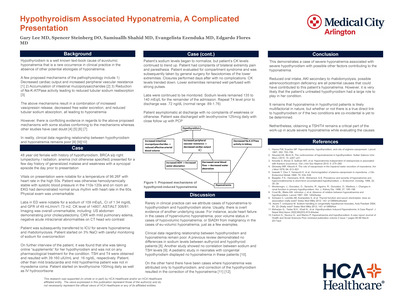
INTRODUCTION: Starvation ketoacidosis represents a rare but complicated maternal morbidity that primarily occurs in the third trimester of pregnancy. With increased insulin resistance and metabolism manifesting in pregnancy, prompt care is required to diagnose and treat starvation ketoacidosis as it appears at an accelerated rate. However, despite the severity of maternal and fetal complications arising from this condition, standardized treatment protocols have not been elucidated. CASE PRESENTATION: In this case report, a 33-year-old gravida 3 para 0-2-0-2 at 31 weeks and 5 days gestational age was admitted to antepartum services for intractable nausea, vomiting, and anuria and transferred to the intensive care unit (ICU) on hospital day 3 for starvation ketoacidosis. Prior to ICU transfer, the patient was started on intravenous (IV) Lactated Ringer’s (LR) solution that was transitioned to IV LR with dextrose 5% solution. Laboratory values indicated metabolic acidosis with pH 7.221, partial pressure of CO2 (PaCO2) of 12.9 mmHg, partial pressure of oxygen (PaO2) 91.2 mmHg, and bicarbonate 5.3 mmol/L on arterial blood gas. Serum bicarbonate <10 mmol>/L on comprehensive metabolic panel. In the ICU, IV fluids were converted to IV 5% Dextrose with 8.4% sodium bicarbonate. Anti-emetic regimen of IV Metoclopramide, IV Ondansetron, rectal Promethazine, and IV Famotidine were continued. Despite 12 hours of treatment, serum bicarbonate and clinic status did not change. Two pushes of IV sodium bicarbonate 8.4% 50 mL solution and Clinimix electrolyte solution was initiated. After 19 hours of continuous IV 5% Dextrose with 8.4% sodium bicarbonate containing fluids, serum bicarbonate improved to 18 mmol/L. The patient was transitioned to a clear liquid diet and didn’t require enteral or parenteral nutrition. However, due to category 3 fetal heart tracing and biophysical profile score of 4/10 despite improved maternal clinical status, an emergent cesarean section was performed on hospital day 4. LEARNING POINTS: In this case, successful treatment of starvation ketoacidosis was achieved with dextrose and sodium bicarbonate IV fluids without enteral or parental nutrition in less than 24 hours. Although the pregnancy concluded with an emergent cesarean section, we can extrapolate a potential regimen to treat starvation ketoacidosis. Our protocol underscores the need for early diagnosis with aggressive treatment and highlights prompt adjustment of treatment regimens when clinical status and laboratory values fail to improve. This case will further expand on the scarce case reports of starvation ketoacidosis in pregnancy and shed light on possible standardized treatment regimens for similar patient presentations.
-

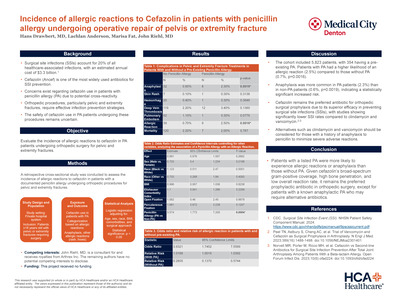
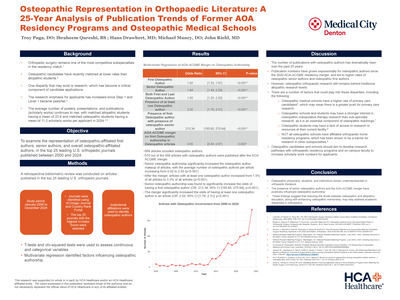
Use of Intraoperative Vancomycin Powder and its Effects on the Incidence of Surgical Site Infection in Orthopaedic Trauma: A Systematic Review and Meta-analysis
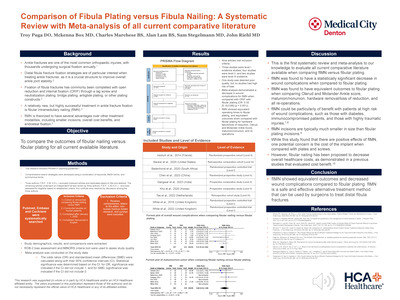
Troy Puga, McKenna Box, Alan Lam, Claire Ferguson, Mason Poffenbarger, Cornelis Potgieter, and John Riel
Introduction Surgical site infection (SSI) in orthopaedic trauma can have devastating consequences for patients. Many risk factors for SSI exist and many strategies are employed to prevent SSI. The use of intraoperative powdered vancomycin is one such strategy used in orthopaedic trauma surgery, however, evidence and guidelines remain unclear. The aim of this systematic review is to evaluate the evidence for the use of powdered vancomycin in orthopaedic trauma surgery for the prevention of SSI. Methods A search was conducted across Pubmed/Medline, Cochrane, and Embase databases to evaluate for the use of powdered vancomycin in orthopaedic trauma surgery for the prevention of SSIs. The search used a combination of keywords and MeSH terms. Titles and abstracts were screened for inclusion criteria eligibility. Full texts were screened and included if they met eligibility criteria. A meta-analysis was completed in order to evaluate the effects of vancomycin in orthopaedic trauma surgery for the prevention of SSIs. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) standards were followed. Results Eight studies met final inclusion criteria for this systematic review. Three were level I evidence studies, and the remaining five were level III evidence studies. Five of the eight studies found a statistically significant reduction in either surgical site/fracture-related infection or reduction in gram-positive SSIs. No studies found any effect on the rate of gram-negative infections. Meta-analysis demonstrated a decrease in overall SSI when powdered vancomycin was used [Odds Ratio (OR) = 0.49 (95% Confidence Interval (CI): 0.33–0.72), P = 0.0003] and a decrease in the incidence of gram-positive SSI [OR = 0.35 (95% CI: 0.14–0.84), P = 0.0185]. Conclusion Powdered vancomycin is a safe and effective treatment option that reduces the rate of overall SSI and gram-positive SSI in orthopaedic trauma surgery patients. However, powdered vancomycin does not reduce gram-negative SSI in orthopaedic trauma patients. There was also no evidence that powdered vancomycin demonstrated any increase in the rates of aseptic wound complications, fracture non-union, or impaired fracture healing. Powdered vancomycin can be safely used in the orthopaedic trauma setting to help reduce the incidence of surgical site infections.
-

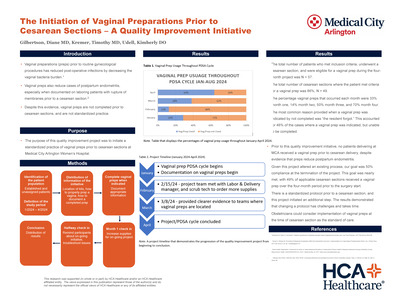
Use of VA ECMO in Patients with Acute Pulmonary Embolism Presenting with Obstructive Cardiogenic Shock undergoing Mechanical Thrombectomy
Luke Taylor, Otoniel Espinoza, Omar O. Hernandez, Shannon Biggers, Shirin Miller, Srinivas Yallapragada, Amer Alaiti, Andrew Fredericks, Song Li, and Claudius Mahr
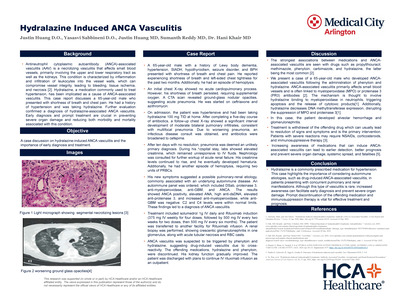
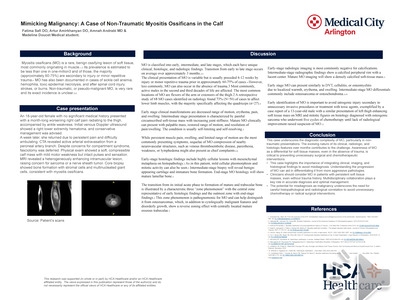
BACKGROUND: Management of VA ECMO has substantially evolved over the years. Much literature has been published regarding indications, management, and outcomes; however, limited evidence exists detailing strategies to manage, progress, and wean patients from VA ECMO. We present our experience using a VA ECMO expected progression patient management guideline. METHODS: The VA ECMO Expected Progression Patient Management Guideline, approved on June 1, 2021, consists of six goal-oriented stages with suggestive interventions for managing cardiogenic shock patients undergoing VA ECMO therapy. Patient characteristics and outcomes were collected retrospectively and compared between March 2019 to May 2021 (VA Non-Expected Progression group) and June 2021 to February 2024 (VA Expected Progression group). RESULTS: Patient characteristics and outcomes are shown in Table 1. Of 93 adult patients, 75 followed the VA ECMO expected progression patient management guideline. There was no significant difference in age, ethnicity, and BMI. Pre-ECMO characteristics were evenly distributed except with at least one inotrope and SAVE score variable in the VA Non-Expected group. Mean ECMO duration, ICU length of stay (LOS), and hospital LOS were shorter in the VA Expected Progression group. Hospital discharge outcome measures demonstrated an increase of 18% in the VA Expected Progression group. Conclusion: This management guideline is a helpful tool that has resulted in streamlined care, shorter ECMO runs, decreased LOS, and improved outcomes. Further studies with adequate sample size are needed to evaluate the effect of protocol implementation on length of stay and survival.
-

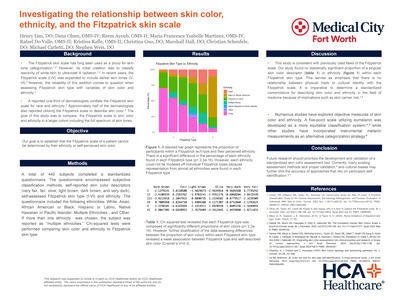
Use of VA ECMO in Patients with Acute Pulmonary Embolism Presenting with Obstructive Cardiogenic Shock undergoing Mechanical Thrombectomy
Luke Taylor, Otoniel Espinoza, Omar O. Hernandez, Shannon Biggers, Shirin Miller, Srinivas Yallapragada, Amer Alaiti, Andrew Fredericks, Song Li, and Claudius Mahr
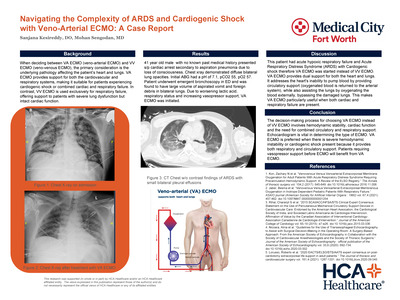
Background Patients with massive/sub-massive pulmonary embolism (PE) and right ventricular strain have a significant risk of hemodynamic collapse. VA ECMO support provides an excellent salvage option for patients with acute/unstable pulmonary embolism with obstructive cardiogenic shock undergoing mechanical thrombectomy. Using VA-ECMO for a “protective PE” procedure allows control of hemodynamics and enables interventionalists to perform the thrombectomy in a more controlled environment. Here, we present our experience. Methods A retrospective data analysis on consecutive VA ECMO patients with cardiogenic shock secondary to pulmonary embolism was abstracted from August 2022 to June 2024. Results Patient characteristics and outcomes are described in Table 1. A total of 19 patients met inclusion criteria. The mean age is 46.3, and the majority of the population was male, 57.9%. Predisposing factors for PE were evenly distributed. Cardiac arrest was present in 57.9% of patients; mean lactate was 8.1, and 68.4% of patients required at least two vasopressors. The mean Survival After Veno-Arterial ECMO (SAVE) score was -4.7. Fifteen out of nineteen patients (79%) survived hospital discharge. Despite correction of metabolic derangements, four patients (21%) expired on ECMO due to anoxic injury related to prolonged CPR. Conclusion The concomitant use of VA ECMO and mechanical pulmonary thrombectomy demonstrated to be an effective treatment modality for massive PE with cardiogenic shock. This combination of therapies allows interventionalists to perform protective thrombectomies in highly acute patients with better hemodynamic control while on ECMO.
-

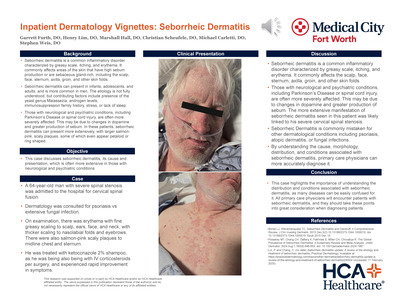
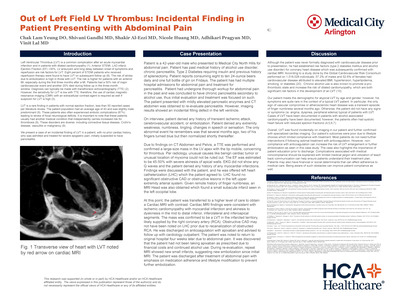
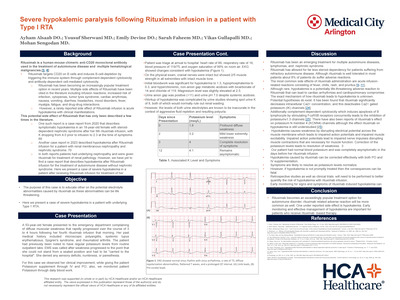
Warm Autoimmune Hemolytic Anemia Camouflaged as Persistent Anemia Post-Embolization for Abnormal Uterine Bleeding: A Case Report
Nischal Pokhrel and Sathish Karmegam
This case report presents a 42-year-old female with heavy menstrual bleeding and syncope, initially diagnosed with AUB due to fibroids. The patient's hemoglobin (Hb) dropped from 11.8 g/dl to 7.3 g/dl within three days, despite multiple PRBC transfusions. Uterine artery embolization (UAE) was performed, but Hb levels continued to decline, prompting further investigation. Additional testing revealed normal iron studies, vitamin B12, and folic acid levels. The peripheral blood smear showed mild anisocytosis, and the ANA screen was negative. However, elevated lactate dehydrogenase (LDH) at 571 U/L, a positive DAT for IgG, and a reticulocyte count of 6.37 were observed. These findings were consistent with warm autoimmune hemolytic anemia (AIHA). Treatment with prednisone 60 mg/day was initiated, and subsequent transfusions used the least incompatible blood units. The patient was discharged with an improved Hb of 9.1 g/dl. Discussion: This case highlights the importance of considering AIHA in patients with persistent anemia, even when an apparent cause like AUB is present. The failure to achieve an adequate rise in Hb despite multiple transfusions was a key clue prompting further investigation. Elevated LDH and reticulocyte count, along with a positive DAT, are characteristic findings of warm AIHA. The overlapping etiology of anemia in this case presented a diagnostic challenge. AUB causes anemia through blood loss, while AIHA results from immune-mediated destruction of red blood cells (RBCs). The anemia from AUB may mask the hemolytic component of AIHA, making differentiation between the two causes difficult. Reticulocytosis, typically seen in AIHA, may be attributed to the body's response to blood loss rather than hemolysis. Elevated LDH and bilirubin levels, common in AIHA, might be less pronounced or overlooked in the context of recent blood loss. Characteristic AIHA findings like spherocytes or polychromasia may be less prominent when concurrent blood loss anemia is present. The smear may appear more consistent with iron deficiency anemia, which is common in chronic AUB. Misdiagnosis as simple blood loss anemia may result in inappropriate management, such as unnecessary iron supplementation or blood transfusions, which can exacerbate hemolysis in AIHA. In conclusion, diagnosing AIHA in the setting of anemia secondary to AUB requires a high index of suspicion, comprehensive laboratory evaluation, and careful clinical correlation. The possibility of masked AIHA should be considered in cases of persistent or worsening anemia despite adequate management of AUB. Early recognition and appropriate management of both conditions are crucial for optimal patient outcomes.
-

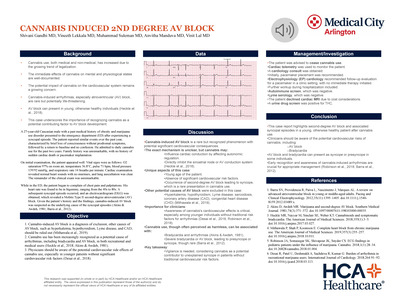
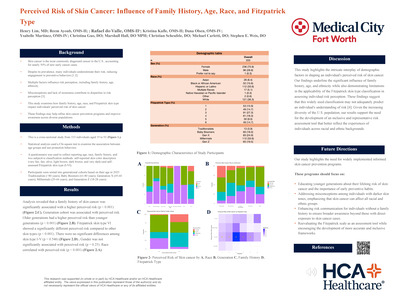
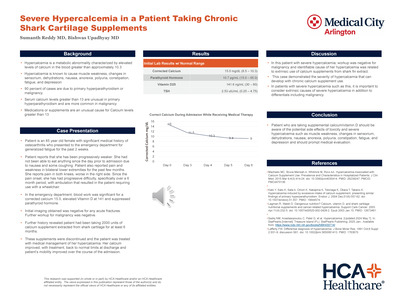
When Skin Necrosis Mimics: Diagnostic and Therapeutic Challenges of Calciphylaxis in a CKD Patient with a Mechanical Heart Valve
Sienna Luk, Harshil Parekh, Vaishnavi Singh, Darshan Bhatty, and Sathish Karmegam
Calciphylaxis is a rare but serious condition characterized by the calcification and thrombosis of small blood vessels, predominantly affecting patients with end-stage renal disease (ESRD). Diagnosis can be challenging due to overlapping features with other vascular conditions, such as warfarin-induced skin necrosis (WSN). We present a case of a patient with ESRD and typical risk factors—peritoneal dialysis, hyperparathyroidism, and warfarin use—who exhibited classic skin findings suggestive of calciphylaxis. However, two skin biopsies were inconclusive. Management involved addressing the patient's calciphylaxis risk factors, optimizing dialysis, and initiating sodium thiosulfate therapy. The case was further complicated by the need to replace warfarin, as current guidelines only approve its use for patients with mechanical heart valves.
-

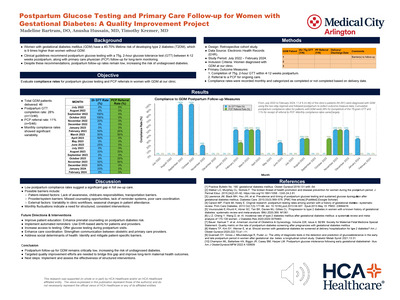
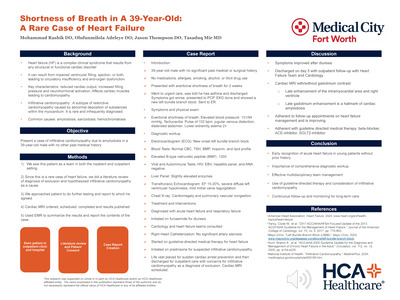
When the Chest and Heart Connect: A Rare Case Presentation of Left Ventricular Pseudoaneurysm
Victor DelPrincipe, Aditya Sharma, Wendy Phillips, Malik Amir, and Sanjeev Nair
We present a rare case of left ventricular pseudoaneurysm (LVPA) resulting from a prior cavity that persisted after surgical treatment of empyema via video-assisted thoracoscopic surgery (VATS) that ultimately lead to chronic inflammation of pericardium, resulting in obtuse marginal artery occlusion causing pseudoaneurysm. Computed tomography angiography (CTA) of the chest suggested that this cavity may have intermittently formed a fistula with the left ventricle, contributing to blood loss and progressive pseudoaneurysm formation. The case highlights the complex interplay between thoracic structures and cardiac pathology in the development of LVPA, with diagnostic and therapeutic challenges addressed.