


North Texas GME Research Forum 2026
Files
Download Full Text (520 KB)
Division
North Texas
Hospital
Medical City Arlington
Specialty
Internal Medicine
Document Type
Poster
Publication Date
2026
Keywords
tuberculosis, disseminated tuberculosis, diagnosis
Disciplines
Bacterial Infections and Mycoses | Internal Medicine | Medicine and Health Sciences
Abstract
Introduction: Tuberculosis (TB) is an insidious pulmonary infection that is most prevalent in developing countries. Primary TB may also become latent after initial infection and remain dormant in the body until the patient becomes immunocompromised. The infection will then resume and can become disseminated, moving hematogenously and through the lymphatics to other areas of the body. Disseminated TB is known to manifest in a variety of ways, making it difficult to diagnose.
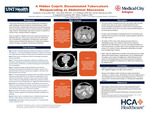
Case Presentation: A 28-year-old- male patient presented to Medical City Arlington with complaints of left lower quadrant abdominal pain. He immigrated from Cameroon 4 years prior. Initial CT imaging showed a rim-enhancing abdominal abscess, sub-capsular collections along the liver, and free fluid in the abdomen. CT angiogram revealed an 8 mm density in the right upper lung lobe, adjacent edema and enlargement of the right pectoralis major muscle, and right parasternal abscess with areas of cortical destruction of the body of the sternum. On day 3, repeat CT demonstrated comparable multiple intra-abdominal, liver, peritoneal, and right pectoral intramuscular abscesses with extension into the anterior mediastinum. On day 4, CT-guided drainage of the right perihepatic fluid collection was performed. Paracentesis fluid was classified as exudative and cultures showed no organisms. On day 5, imaging showed high-grade small bowel obstruction, likely secondary to multiple abdominal abscesses. Exploratory laparotomy was performed with extensive lysis of adhesions and abdominal organ and lymph node resections. Preliminary histopathology of abdominal specimens showed caseating and noncaseating granulomas, suggestive of disseminated TB. The following day, MRI was significant for diffuse osteomyelitis of the sternum with infectious myositis of the right pectoralis major muscle. Thus, a drainage of the right pectoralis fluid collection was conducted. On day 8, a Quantiferon-TB Gold test was shown to be positive, suggesting disseminated TB. On day 12, the patient was initiated on RIPE therapy. After a few weeks, peritoneal fluid AFB PCR and culture were positive for TB.
Learning Points: Because of its ability to infect virtually any organ and therefore manifest in a variety of ways, TB should be on the list of differentials in any individual with a history that predisposes them to TB such as recent travel or immunocompromisation. The ability of TB to mimic other disease processes leads to a challenging workup. This case highlights the importance of a high clinical suspicion as well as an awareness for these niche cases of extrapulmonary presentation.
Original Publisher
HCA Healthcare Graduate Medical Education
Recommended Citation
Veerareddy, Sudiksha; Hall, Alex; Sakhuja, Urvi; Abuelayyan, Sarah; Ezenduka, Evangelista; and Varghese, Rinu, "A Hidden Culprit: Disseminated Tuberculosis Masquerading as Abdominal Abscesses" (2026). North Texas GME Research Forum 2026. 29.
https://scholarlycommons.hcahealthcare.com/northtexas2026/29