

Division
East Florida
Hospital
HCA Florida Palms West Hospital
Specialty
Pediatrics
Document Type
Poster
Publication Date
2023
Keywords
rash, emesis, pancytopenia
Disciplines
Hemic and Lymphatic Diseases | Medicine and Health Sciences | Pediatrics | Virus Diseases
Abstract
Introduction: This is a case of a patient presenting with fever, rash, and vomiting. Upon further studies, patient was found to have pancytopenia which started an extensive hospital work up.
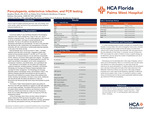
Case Description: A previously healthy 9- year-old female presented to the emergency department with 3 days of tactile fever, 2 days of rash, and 1 day of nonbilious nonbloody emesis. The rash initially appeared on the trunk and by the day of admission, had begun to spread peripherally to the extremities. The rash on the abdomen was described as mild, generalized, blanchable and maculopapular. The rash on the extremities was described as mild, nonblanching, and maculopapular on the lower extremities with mild, erythematous, nonblanchable petechiae bilaterally on the soles of the hands and feet. Initial labs in the ED showed a complete blood count significant for anemia, leukopenia, thrombocytopenia, bandemia, and an ANC of 2847. Complete metabolic panel and uric acid were within normal limits. There was, however, an elevated lactate dehydrogenase and c-reactive protein. Coagulation studies were ordered and demonstrated elevated PT and INR, but PTT was within normal limits. UA showed proteinuria, but was otherwise unremarkable. COVID, Influenza, and Group A Strep swabs were negative. The patient was given Ibuprofen, Ondansetron, and Diphenhydramine in the ED. The patient was admitted to the pediatric unit for further management of pancytopenia, bandemia, acute febrile illness, and a generalized rash.
Upon admission to the pediatric unit, the patient was initially given supportive treatments, including probiotics, Famotidine, and Ibuprofen. Hematology and Oncology and Infectious Disease Specialists were consulted for further management. The Hematology and Oncology Specialist ordered a hematologic workup, which demonstrated a positive Von Willebrand Antigen of 218%, but Fibrinogen, Factor VII, Factor VIII, Factor XIII, and Von Willebrand factor ristocetin cofactor were all within normal limits. The Infectious Diseases Specialist recommended we start the patient on Doxycycline as empiric therapy while awaiting further results, including a full respiratory viral panel. The results demonstrated the patient was positive for Enterovirus and CMV IgG antibodies but negative but CMV IgM antibodies and antinuclear antibodies. Patient continued to be febrile 2 days post admission, which led us to start the patient on Ceftriaxone per Infection Disease recommendation. In due course, Ceftriaxone was discontinued after the patient was afebrile for 2 days and Doxycycline was discontinued after blood culture demonstrated no growth for 3 days. By time of discharge, blood, throat, and stool cultures indicated no growth. Strep screen, Influenza, and SARS-COV-2 NAA were all negative. Upon day of discharge, the patient was afebrile and stable with no emesis, generalized rash improving, pancytopenia improving, and appropriate PO intake.
Discussion: Pancytopenia can be associated with a wide range of diseases, some of which can be life-threatening. While it is a commonly known fact that certain viral infections can cause pancytopenia, our case study shows that enterovirus can cause pancytopenia. If a patient presents with pancytopenia and a rash that involves palms and soles of feet, keep enterovirus in the differential. Enterovirus infection can also have a wide range of disease processes and in some cases be life-threatening, especially if it affects the central nervous system, heart, or liver. It is important to perform a careful history and physical exam as well as acquire appropriate additional studies and consultations. None of the authors have any financial interests, relationships or affiliations relevant to the subject of this manuscript. This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Recommended Citation
Mock, Stephen; Herzstein, Salome; and Horbey, Andrea, "Pancytopenia, enterovirus infection, and PCR testing" (2023). East Florida Division GME Research Day 2023. 31.
https://scholarlycommons.hcahealthcare.com/eastflorida2023/31
Abstract