


North Texas GME Research Forum 2026
Files
Download Full Text (465 KB)
Division
North Texas
Hospital
Medical City Arlington
Specialty
Internal Medicine
Document Type
Poster
Publication Date
2026
Keywords
orthotopic heart transplantation, OHT, advanced heart failure, antibody-mediated rejection, graft dysfunction
Disciplines
Cardiology | Cardiovascular Diseases | Internal Medicine | Medicine and Health Sciences | Surgical Procedures, Operative
Abstract
INTRODUCTION: Orthotopic heart transplantation (OHT) remains the gold standard treatment for patients with advanced heart failure refractory to optimal medical and device-based therapies. Despite advances in perioperative management, immunosuppressive regimens, and long-term surveillance protocols, graft rejection remains a major determinant of post-transplant morbidity and mortality [1]. We report a case, representing one of the longest documented intervals in literature, of suspected antibody-mediated rejection (AMR) occurring 23 years after heart transplantation in which conventional endomyocardial biopsy (EMB) could not be successfully performed. This case highlights the diagnostic uncertainty associated with very late AMR and underscores the potential role of clinical presentation, immunologic biomarkers, and advanced imaging modalities in guiding diagnosis and management when histopathologic confirmation is not feasible.
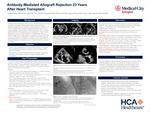
CASE PRESENTATION: A 73-year-old man with a history of OHT presented for evaluation of suspected antibody-mediated rejection (AMR), reflected by elevated class II donor-specific antibodies (DSA) and a Donor-derived cell-free DNA (dd-cfDNA) assay score of 0.4. He had no prior history of rejection or graft dysfunction. His immunosuppression regimen included sirolimus and mycophenolate mofetil. EMB was attempted and unsuccessful twice. Transthoracic echography and cardiac MRI revealed moderate left ventricular dysfunction and severely dilated atria. MRI showed marked LA enlargement (9.2 x 9.4 cm) and moderate-to-severe RA dilation, with prolonged T2 signals (59 msec) (Figures). Left heart catherization revealed a 40% stenosis of the left anterior descending artery, consistent with Grade 1 CAV. He was treated for presumed AMR with plasmapheresis, IV immunoglobulin, high-dose corticosteroids, anti-thymocyte globulin, and adjustment of immunosuppression regimen.
DISCUSSION: AMR is a feared complication of solid organ transplantation [2]. Etiology is likely multifactorial, involving postoperative structural changes and possible subclinical immunologic injury leading to fibrosis and impaired atrial compliance. The interactions between humoral and cellular immunity in chronic allograft dysfunction is complicated making clinicians unable to depend on a single marker as a sole indicator of rejection [3]. EMB is the gold-standard but they are invasive, carry risks, and can be done a limited amount of times [4,5]. Cardiac MRI is emerging as a comprehensive assessment of function, morphology, and tissue characterization without these risks [6].
CONCLUSION: Patients with long-term OHT may develop chronic graft dysfunction secondary to AMR despite being asymptomatic, showing the importance of regular surveillance. Cardiac MRI may detect dysfunction missed by echocardiography. Our findings underscore the importance of integrating clinical presentation, advanced imaging, and emerging biomarkers to support diagnosis and management when EMB is not feasible.
Original Publisher
HCA Healthcare Graduate Medical Education
Recommended Citation
Parmar, Jorim; Lapsiwala, Boney; Adusumilli, Devika; Luk, Sienna; Dung, Nguyen; Li, Song; and Tamirisa, Kamala, "Antibody-Mediated Allograft Rejection 23 Years After Heart Transplant" (2026). North Texas GME Research Forum 2026. 26.
https://scholarlycommons.hcahealthcare.com/northtexas2026/26
Included in
Cardiology Commons, Cardiovascular Diseases Commons, Internal Medicine Commons, Surgical Procedures, Operative Commons