


North Texas GME Research Forum 2026
Files
Download Full Text (751 KB)
Division
North Texas
Hospital
Medical City Fort Worth
Specialty
Internal Medicine
Document Type
Poster
Publication Date
2026
Keywords
acute pancreatitis, AP, hyper-triglyceride induced acute pancreatitis
Disciplines
Digestive System Diseases | Gastroenterology | Internal Medicine | Medicine and Health Sciences
Abstract
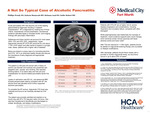
BACKGROUND Acute pancreatitis (AP) has become one of the leading gastrointestinal diagnoses resulting in inpatient hospitalization¹. AP is diagnosed by meeting two of three criteria: characteristic clinical presentation, biochemical evidence (elevated lipase or amylase levels), and imaging findings with pancreatic inflammation. Gallstones and heavy alcohol use account for most cases (40%–70% and 25%–35%, respectively). Hypertriglyceride induced AP (HTG-AP) accounts for only about 7-10% of AP cases³ and often tends to present in younger, male, obese, patients with a higher rate of diabetes¹. Below we present a unique case of a coinciding alcoholic and HTG - AP in an otherwise healthy female and discuss the importance of early diagnosis and appropriate treatment.
CASE DESCRIPTION The patient is a 56-year-old woman with a history of alcohol use disorder and scoliosis who presented with epigastric pain, nausea, and vomiting. She reported drinking twelve 12-oz beers daily and had one prior hospitalization for alcohol-related pancreatitis earlier this year. Lipase on admission was 632 U/L, and abdominal MRI showed peripancreatic edema consistent with AP. Her alcohol level was elevated which further supported alcoholic pancreatitis. To complete the AP workup, triglyceride (TG) level was collected and found to be markedly elevated at 2740 mg/dL. The patient was promptly admitted and started on an insulin drip with 87% TG reduction within 24 hours. She was then transitioned to fenofibrate and discharged on orlistat, fenofibrate, and dietary modifications.
DISCUSSION Patients with HTG-AP are at higher risk for severe disease progression and complications, including respiratory and circulatory failure, compared with other etiologies⁴. While plasmapheresis was traditionally the mainstay of treatment, recent evidence supports early insulin therapy, which achieves similar clinical outcomes with fewer adverse events and lower costs⁵. After TGs are reduced to < 1,000 mg/dL, patients should be started on triglyceride-lowering therapy and counseled on lifestyle modifications. After discharge, patients should follow closely with a provider to monitor triglyceride levels, as recurrence occurs in up to about 20% of cases².
Original Publisher
HCA Healthcare Graduate Medical Education
Recommended Citation
Phillips, Wendy; Munazzah, Kaleem; Rehman, Asad; and Keller, Robert, "A Not So Typical Case of Alcoholic Pancreatitis" (2026). North Texas GME Research Forum 2026. 65.
https://scholarlycommons.hcahealthcare.com/northtexas2026/65