


North Texas GME Research Forum 2024
On April 19, 2024, Medical City Arlington hosted the North Texas Division Research Forum with 200+ attendees (in-person & virtual), over 300 authors, 12 oral presentations, 34 in-person poster presentations, and 52 virtual poster presentations celebrating scholarly activity from the North Texas Regional Consortium of Medical City Healthcare, University of North Texas (UNT), and Texas Christian University (TCU). The forum was honored to have Dr. Song Li of Advanced Heart Failure and Transplant Cardiology and Director of Cardiogenic Shock at Medical City Dallas. He spoke about “Machine Learning and Artificial Intelligence in Healthcare”.
Research Category Winners
- 1st - Bradley Gustafson; Nasima Mehraban, Amjad Awan from Medical City Arlington Internal Medicine, Comparing the Positive Predictive Value of At-Home Screening Tests with Chronic Anticoagulant and/or Antiplatelet Therapies
- 2nd - Neil Werthmann; Mason Poffenbarger; John Riehl from Medical City Denton Orthopedic Surgery, Comparison of Three Treatments for Fractures of the Humeral Shaft
- 3rd - Chrystal Stallworth; Abel Moron; Nicole Tenzel; Timothy Kremer; Michele McCarroll from Medical City Arlington OBGYN, Surgical Margin Analysis in Early-Stage Cervical Cancer: An HCA Healthcare Retrospective Study
Quality Improvement Category Winners
- 1st - Ariel Moskowitz; Nicole Tenzel; Joshua Mangels; Lyndsay Millican from Medical City Arlington OBGYN, Implementing a Standardized Screening Algorithm for Iron Deficiency Anemia in Pregnancy
- 2nd - Jennifer Austin; April Miller; Alicia Lay from Medical City Plano General Surgery, Multidisciplinary Simulation-Based Trauma Education for General Surgery Interns
- 3rd - Zachary Shields; Enrique Alvarez-Ventura; Curtis Johnson from Medical City Arlington Emergency Medicine, Impact of Vertical Zone Redesign: One Hospitals Experience
Case Report Category Winners
- 1st - Jennifer Austin; Enrique Alvarez-Ventura; Alicia Lay; Christian Minshall from Medical City Plano General Surgery, Survival After Emergency Clamshell Thoracotomy with Bilateral Atrial Appendage Injuries
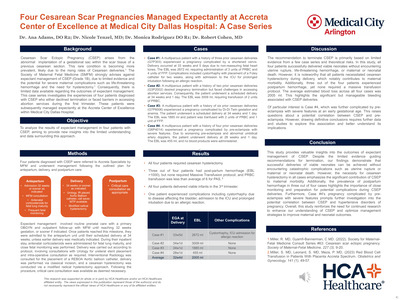
- 2nd - Ana Adams; Monica Rodriguez; Robert Cohen from Medical Cuty Arlington OBGYN, Four Cesarean Scar Pregnancies Managed at Accreta Center of Excellence at Medical City Dallas Hospital: A Case Series
- 3rd - Raleigh Payton; David Bassa; Furrukh Jabbar; Hassan Ahmad from Medical City Plano General Surgery, Primary Resection of Duodenal Neuroendocrine Tumor with Suspected Lymph Node Metastasis: A Case Report
Overall Research Forum Winner (Most Votes):
- Chrystal Stallworth from Medical City Arlington OBGYN, Surgical Margin Analysis in Early-Stage Cervical Cancer: An HCA Healthcare Retrospective Study
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-

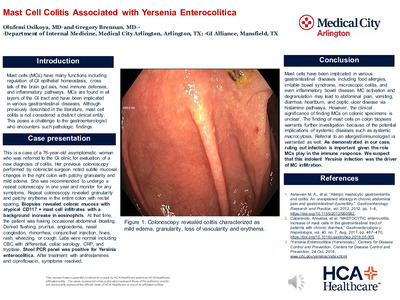
Mast Cell Colitis Associated With Yersinia Enterocolitica
Olufemi Osikoya and Gregory Brennan
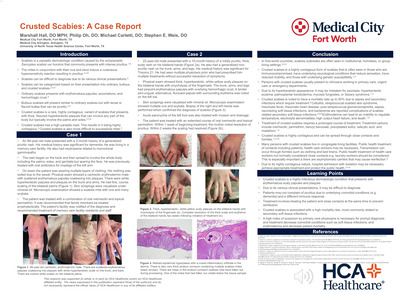
Introduction: Mast cells (MCs) have many functions including regulation of GI epithelial homeostasis, cross talk of the brain gut axis, host immune defenses, and inflammatory pathways. MCs are found in all layers of the GI tract and have been implicated in various gastrointestinal diseases. Although previously described in the literature, mast cell colitis is not considered a distinct clinical entity. This poses a challenge to the gastroenterologist who encounters such pathologic findings. Case Presentation: This is a case of a 76-year-old woman who was referred to the gastroenterology clinic for evaluation of a new diagnosis of colitis. The patient had undergone a routine colonoscopy by a colorectal surgeon who had noted subtle mucosal changes in the right colon including patchy granularity and mild edema. The patient was asymptomatic, and therefore, it was recommended she undergo a repeat colonoscopy in one year and monitor for any symptoms. Repeat colonoscopy, one year later, revealed granularity and patchy erythema in the entire colon with rectal sparing. Biopsies revealed colonic mucosa with atypical CD117 + mast cell infiltrates with a background increase in eosinophils. At that time, the patient was having occasional abdominal bloating. She denied flushing, pruritus, angioedema, nasal congestion, rhinorrhea, conjunctival injection, hives, rash, wheezing, or cough. Laboratories were normal including CBC with differential, celiac serology, CRP, tryptase. Stool PCR panel was positive for Yersinia enterocolitica. The patient was treated with antihistamines and ciprofloxacin and her symptoms resolved. Learning Points: Mast cells have been implicated in various gastrointestinal diseases including food allergies, irritable bowel syndrome, microscopic colitis, and even inflammatory bowel disease. MC activation and degranulation may lead to abdominal pain, vomiting, diarrhea, heartburn, and peptic ulcer disease via histamine pathways. However, the clinical significance of finding MCs on colonic specimens is unclear. The finding of mast cells on colon biopsies warrants further investigation because of the potential implications of systemic diseases such as systemic macrocytosis. Referral to an allergist/immunologist is warranted as well. As demonstrated in our case, ruling out infection is important given the role MCs play in the immune response. We suspect that this indolent Yersinia infection was the driver of MC infiltration.
-

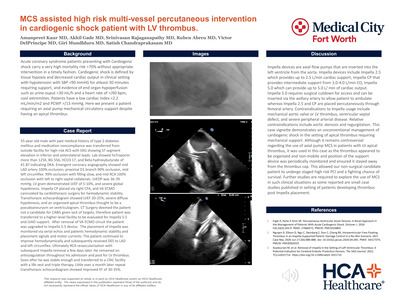
MCS Assisted High Risk Multi-Vessel Percutaneous Intervention in Cardiogenic Shock Patient with LV Thrombus
Amanpreet Kaur, Akhil Gade, Srinivasan Rajaganapathy, Ruben Abreu, and Victor DelPrincipe
Background: Acute coronary syndrome patients presenting with Cardiogenic shock carry a very high mortality risk >70% without appropriate intervention in a timely fashion. Here we present a patient requiring an axial pump mechanical circulatory support despite having an apical thrombus. Case report: 55-year-old male with past medical history of type 2 diabetes mellitus and medication noncompliance was transferred from outside facility for high risk ACS with EKG showing ST segment elevation in inferior and anterolateral leads. Lab showed hsTroponin more than 125K, BG 556, HCO3 17, and Beta hydroxybutyrate of 41.87 indicating DKA. Emergent coronary angiography showed mid LAD artery 100% occlusion, proximal D1 branch 90% occlusion , mid left circumflex 99% occlusion with filling slow, and mid RCA 100% occlusion with left to right septal collaterals. LVEDP was 36-39 mmHg. LV gram demonstrated LVEF of 5-10%, and severe global hypokinesis. Impella CP placed via right CFA, and VA ECMO cannulated by cardiothoracic surgery for hemodynamic stability. Transthoracic echocardiogram showed LVEF 20-25%, severe diffuse hypokinesis, and an organized apical thrombus thought to be a pseudoaneurysm on ventriculogram. CT Surgery deemed the patient not a candidate for CABG given lack of targets, therefore patient was transferred to a higher level facility to be evaluated for Impella 5.5 and LVAD support. After removal of VA ECMO circuit and upgrade to Impella 5.5 device, the patient continued to improve hemodynamically and subsequently received DES to LAD and left circumflex. Ultimately RCA revascularization with subsequent impella removal a few days later. He remained on anticoagulation throughout his admission and post for LV thrombus. Soon after he was stable enough and transferred to a LTACH facility with a life vest and triple therapy. Little over a month later repeat transthoracic echocardiogram showed improved EF of 30-35%. Discussion: This case vignette demonstrates an unconventional management of cardiogenic shock in the setting of apical thrombus requiring mechanical support. Although it remains controversial regarding the use of axial pump MCS in patients with LV apical thrombus, it was used in this case as the thrombus was considered to be organized and non mobile and position of the support device was periodically monitored and ensured it stayed away from the thrombus cap. This allowed our high risk non surgical candidate patient to undergo staged high risk PCI and a fighting chance of survival. Further studies are required to explore the use of MCS in such clinical situations.
-

Multidisciplinary Management for Large and Difficult Choledocholithiasis: The Role of Choledochotomy
Jilpa Shah and Balu Chandra
Extracranial carotid artery aneurysm is a rare sequela of atherosclerosis, trauma, and conditions of chronic inflammation. Standard treatments include antiplatelet medications, open resection, or endovascular stenting. Transcarotid artery revascularization (TCAR) has become a well-recognized alternative treatment in the past few decades. This case study documents the first reported case of Horner’s syndrome post-TCAR for an internal carotid artery (ICA) aneurysm. A 68 year-old male with intermittent double vision was referred to vascular surgery clinic with brain CT angiography showing a 9mm saccular aneurysm with dissection flap of the right cervical ICA. Prior attempts by neuro-interventional radiology were unsuccessful due to tortuous anatomy. After lengthy discussion with the patient, the decision was made to proceed with TCAR. The TCAR procedure was conducted with flow reversal from the right common carotid artery (CCA) to the left femoral vein. A Iliac covered stent, arterial stent was used to stent the lesion. Angiography demonstrated a small dissection at the cavernous segment of the internal carotid artery (ICA). A second stent was placed across the dissection. The completion angiogram showed no residual lesions. Patient was monitored in the ICU postoperatively. A few hours following the procedure, the patient began to complain of a significant frontal headache despite strict blood pressure control. A CT head was completed without any acute findings. Post-op day 1, the patient developed Horner’s syndrome with symptoms of mild right eye ptosis, anisocoria with excessive right eye tearing, and flushing of the face. Post-op day 2, the patient remained stable with persistent Horner’s symptoms. The patient was discharged with tapered methylprednisolone sodium succ regimen with planned close follow up in the clinic. At two-week follow-up, the patient’s symptoms had nearly resolved Horner’s syndrome has been documented as a rare complication following other endovascular carotid procedures. Stretching of the sympathetic fibers that course along the carotid artery is thought to be the cause of this rare complication. Treatment is generally supportive, but there has been documented cases of steroid use. The case highlighted describes a rare and previously undocumented complication of TCAR in high carotid artery lesions. This case will further help understand the possible complications of performing the TCAR procedure and assist in patient selection and treatment discussions for future carotid artery lesions.
-

Multidisciplinary Simulation-Based Trauma Education for General Surgery Interns
Jennifer Austin, April Miller, Jeremiah Avarana, and Alicia Lay
Introduction: According to the American Society of Gastroenterology Endoscopy (ASGE), choledocholithiasis is defined as the presence of gallstones in biliary tree. Choledocholithiasis is concomitantly present in approximately 1 to 10 percent of patients with cholelithiasis. Choledocholithiasis can be described as small <15>mm, large >15 mm, and difficult due to anatomic location, impaction, or unusual hardness/ shape. Choledocholithiasis is managed endoscopically with large balloon papillary dilation, cholangioscopy-guided intraductal laser and electrohydraulic lithotripsy (EHL), and escalation to laparoscopic common bile duct exploration, if endoscopic procedures fail. Thus far, there are sparse studies that show the requirement of choledochotomy in large and difficult choledocholithiasis management. Case: A 55-year-old African-American female with hypertension presented with colicky epigastric and right upper quadrant abdominal pain intermittently for 10 years, which was self-resolving. She presented as hemodynamically stable, mildly leukocytic with elevated liver function tests and dilated common bile duct (CBD). Abdominal ultrasound and Computed Tomography Angiography suggested presence of multiple cholelithiasis and choledocholithiasis. She underwent Endoscopic Retrograde Cholangiopancreatography (ERCP) and biliary sphincterotomy that demonstrated multiple large choledocholithiasis from ampulla of Vater to hilum of liver (Figure 1). No stones were removed due to the large size and hard-to-reach locations. Initially, a 7 cm plastic biliary stent encapsulating the existing stones was placed 6 cm into the CBD. Within three days, the initial biliary stent was found to be partially occluded, and a new stent needed to be placed. Biliary sludge and one stone were removed while multiple stones remained. Endoscopist performed direct visualization of ducts with SPY, which demonstrated multiple stones in the lower third of CBD with the largest measuring 1.8 cm in size. Patient underwent Laparoscopic Cholecystectomy with CBD exploration and Lithotripsy, which was converted into a choledochotomy by a hepatobiliary surgeon. The remaining stones were successfully removed. Post-operatively, the patient was optimized with pain control and Piperacillin/Tazobactam for antibiotic coverage, and discharged 3 days later without postoperative complications. Discussion: Current guidelines published in ASGE, do not explicitly recommend performing surgical intervention of large and difficult choledocholithiasis with choledochotomy. However, this case highlights the necessity for surgical escalation of care for the management of large and difficult CBD stones. Ultimately, more case studies will need to be reported in order to support the utilization of a multidisciplinary approach towards the successful management of large and difficult choledocholithiasis.
-

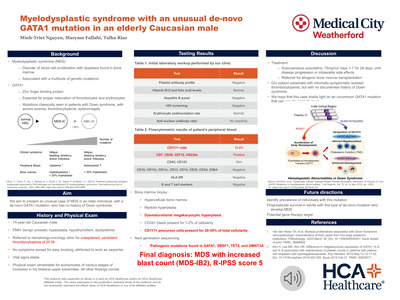
Myelodysplastic Syndrome with an Unusual De-novo GATA1 Mutation in an Elderly Caucasian Male: A Case Report
Minh-Triet Nguyen, Maryam Fallahi, and Talha Riaz
Myelodysplastic syndrome (MDS) is a disorder of blood cell proliferation that has been shown to have multiple risk factors for pathogenesis. One risk factor well documented in existing literature is a mutation in GATA-binding factor 1 (GATA1) which is classically seen in younger individuals with Down syndrome. However, in our case report, we present an unusual presentation of MDS with a de novo GATA1 mutation in a 75-year-old male with no history of Down syndrome, who initially presented with isolaterombocytopenia. A 75-year-old male presented for evaluation of unexplained asymptomatic thrombocytopenia found incidentally on outpatient laboratory evaluation. Further evaluation of the thrombocytopenia revealed an increased (18.8%) proportion of clonal CD117+ cells via flowcytometry, and markedly hypercellular bone marrow with left shifted myeloid hyperplasia and dysmaturational megakaryocytic hyperplasia, consistent with a diagnosis of new onset myelodysplastic syndrome with increased blast count (MDS-IB2). A subsequent next generation sequencing incidentally found a de-novo mutation in GATA1. The patient was placed on azacitidine and was referred to a local bone marrow transplant clinic for further evaluation. The patient does not have a history of Down syndrome and his physical exam was inconsistent with findings typical of the syndrome. He also presented with isolated asymptomatic thrombocytopenia as his first sign of MDS. Although documented cases of GATA1 mutations in younger patients with Down syndrome and MDS have been noted, there exists a paucity of literature in older individuals with this type of presentation. This subset of MDS with GATA1 mutation is of unclear clinical significance in older individuals and may require further investigation, especially regarding prognostication and possible future treatment avenues.
-
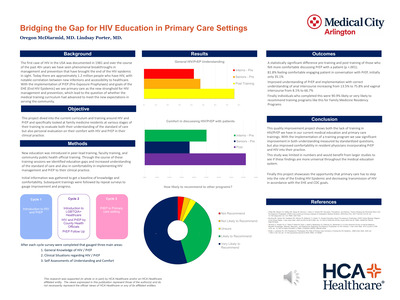
 Utilization in the Primary Care Setting by Ceferino Cruz and Afsha Rais")
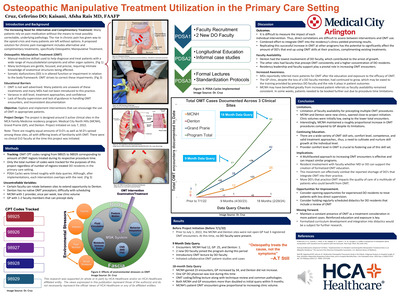
Osteopathic Manipulative Treatment (OMT) Utilization in the Primary Care Setting
Ceferino Cruz and Afsha Rais
INTRODUCTION: Osteopathic Manipulative Treatment (OMT) is a skillset used to help diagnose and treat patients with a wide range of musculoskeletal complaints and can also be used as adjunctive treatment modalities for other organ systems. The project is designed to increase OMT usage across 3 clinical sites in our residency program to improve the quality of care provided to our patients. OBJECTIVES: Integrate OMT review into longitudinal clinical education. Address the shortage of faculty members that can precept OMT across all three sites. METHODS: The metrics being tracked are various OMT CPT codes ranging from 98925 to 98929 at 3 clinic sites: North Richmond Hills (NRH), Grand Prairie (GP), and Denton. Only the total number of codes were used. 2 additional D.O faculty members joined during the data collection period. RESULTS: Prior to July 2022, the NRH and Denton sites were not open, and GP had 3 registered OMT encounters. 12 months post QI implementation demonstrated that OMT usage had increased across all three sites. Between July 1, 2022, and April 30, 2023, NRH registered 12 OMT encounters, GP registered 25, and Denton registered 1. CONCLUSION: Longitudinal education along with increased availability of faculty to precept OMT may have led to the significant increase in OMT encounters. Denton had the least opportunity for faculty to precept OMT. GP had the highest, and NRH had Wednesdays dedicated to OMT procedures, which the data appears to reflect. It is anticipated that with more faculty availability to precept OMT, encounter numbers would increase further. At this time, further data from Fall 2023 onwards is being collected and will be integrated into Phase 2 which will conclude the project.
-

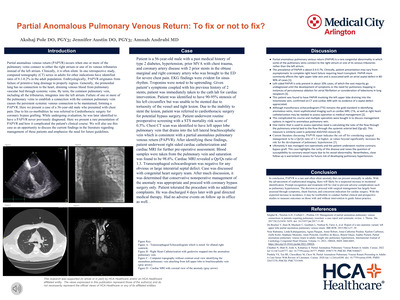
Partial Anomalous Pulmonary Venous Return: To Fix or Not to Fix?
Akshaj Pole, Jennifer Austin, and Amnah Andrabi
Patient is a 56-year-old male with a past medical history of type 2 diabetes, hypertension, prior MVA with chest trauma, and coronary artery disease with 2 prior stents in the obtuse marginal and right coronary artery who was brought to the ED for severe chest pain. Patient was immediately taken to the cath lab for cardiac intervention. Patient was identified to have 90-95% stenosis of his left circumflex but was unable to be stented due to tortuosity of the vessel and tight lesion. Due to patient’s multivessel coronary artery disease and newly diagnosed diabetes, patient was referred to cardiothoracic surgery for potential bypass surgery. Patient underwent routine pre-operative screening with a STS mortality risk score of 0.5%. Chest CT scan was identified to have left upper lobe pulmonary vein that drains into the left lateral brachiocephalic vein which is consistent with a partial anomalous pulmonary venous return (PAPVR). After identifying these findings, patient underwent right sided cardiac catheterization and cardiac MRI for further pre-operative assessment. Transesophageal echocardiogram was negative for any obvious or large interatrial septal defect. The prevalence of PAPVR is about 0.4-0.7%. Clinically, patient presentation may vary from asymptomatic to complete right heart failure requiring heart transplant. PAPVR more commonly affects the right upper lobe vein and is associated with an atrial septal defect in 80-90% of cases. Left-sided PAPVR is only present in about 10% cases, of which the vast majority go undiagnosed until the development of symptoms or the need for pulmonary mapping in instances of percutaneous ablation for atrial fibrillation or consideration of lobectomy in lung neoplasm. Case was discussed with congenital heart surgery team. After much discussion, it was determined that conservative nonoperative management of the anomaly was appropriate and proceed with coronary bypass surgery only. Here we examined a case of an extremely rare presentation of PAPVR originating in the left upper lobe with no evidence of ASD. This anomaly complicated the patient’s course on whether his bypass graft would entail surgical repair of the PAPVR. Recent advancements in sophisticated diagnostic imaging and greater knowledge of this anatomical variation have increased the frequency with which this condition is diagnosed. With the suspected increase in incidence, it may be time for the creation of formal guidelines on a global scale instead of relying on recommendations on consensus of symptomatology.
-

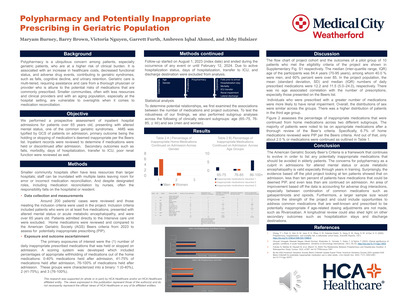
Polypharmacy and Potentially Inappropriate Prescribing in Geriatric Population
Maryam Burney, Barry Brown, Victoria Nguyen, Garrett Furth, Ambreen I. Ahmed, and Abigail Hulsizer
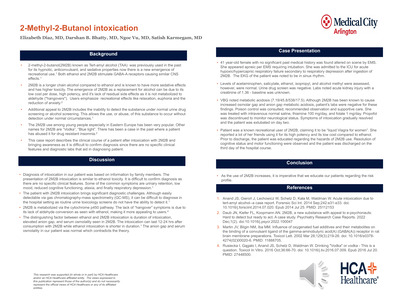
Polypharmacy is a ubiquitous concern among patients, especially geriatric patients, who are at a higher risk of clinical burden. It is associated with an increase in healthcare costs, decreased functional status, and adverse drug events, contributing to geriatric syndromes, such as falls, cognitive decline, and urinary retention. Geriatric care is multi-tiered, requiring assistance and care from a thorough physician who is attune to the potential risks of medications that are commonly prescribed. Smaller communities, often with less resources and clinical providers and with an aging population, especially at the hospital setting, are vulnerable to oversights when it comes to medication reconciliation. We performed a prospective assessment of inpatient hospital admissions for patients over 70 years old, presenting with altered mental status, one of the common geriatric syndromes. Medication records were reviewed and evaluated for inappropriate medications per the Beers Criteria for Potentially Inappropriate Medication Use in Older Adults (BEERS) inpatient records were reviewed to determine if medications were appropriately reviewed and reconciled. The flow chart of study cohort and the outcomes of a pilot group of 10 patients who met the eligibility criteria of the study are shown in Supplementary Fig. S1 respectively. The median (inter-quartile range, IQR) age of the participants was 84.4 years (70-95 years), among whom 40.0 % were men, and 60% percent were over 85. In the study population, the mean (standard deviation, SD) and median (IQR) numbers of daily prescribed medications were 12.2 and 11.5 (5.0–24.0), respectively. There was no age associated correlation with the number of prescriptions, especially those presented on the BEERS. Individuals who were prescribed with a greater number of medications were more likely to have renal impairment. Overall, the distributions of sex were similar across the groups. There was a higher distribution of patients in the third age group. The majority of patients were noted to be on appropriate medications after a thorough review of the BEERS criteria. Specifically, 6.7% of home medications reviewed were PIP per the Beers criteria. And out of that, only about 2.0 % or medications were continued. A larger sample size would improve the strength of the project and could include opportunities to address common medications that are well-known and prescribed to be potentially inappropriate if age-related dosing adjustments are not made, such as Rivaroxaban. A longitudinal review could also shed light on other secondary outcomes such as hospitalization stays and discharge destinations.
-

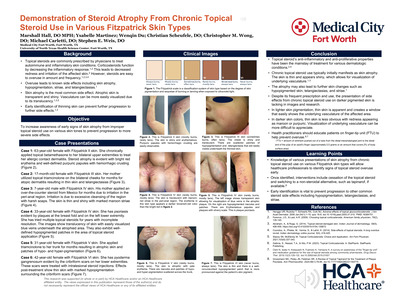
Presentations of Cutaneous Disease in Various Skin Pigmentations: Steroid Atrophy
Marshall Hall, Ysabelle Martinez, Wenqin Du, Christian Scheufele, and Christopher M. Wong
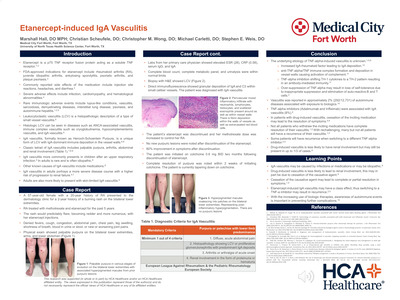
Introduction: Topical steroids are commonly prescribed first-line medications for various inflammatory and autoimmune dermatologic conditions. Their widespread use raises the importance of proper use. Topical steroids have well-known side effects including skin atrophy, redness, striae, and telangiectasias. These side effects have not been well documented in patients of various skin tones. Primary care clinicians must recognize topical steroid side effects and their appearance in various skin tones. This paper will focus on representing skin atrophy, the most common steroid side effect, in a variety of Fitzpatrick skin types. Case Presentation: We present a series of images illustrating skin atrophy after prolonged topical steroid use on various Fitzpatrick skin types. The first case shows Fitzpatrick V skin with areas of erythema, hypopigmentation, and hyperpigmentation on the trunk. The second case presents thin skin with bright erythema and purpuric papules on the upper extremities of Fitzpatrick II skin. A third case shows symmetric, parallel, linear, maroon dermal scars perpendicular to tension lines in the background of epidermal atrophy circum-anally and on the buttocks of Fitzpatrick IV skin. A fourth case exhibits Fitzpatrick III skin with shiny, thin skin and patches of hypopigmentation and telangiectasias on bilateral cheeks. The final case is a Fitzpatrick IV skin type with plaque psoriasis on the lower extremity and a background of skin thinning, hypopigmentation, and visible underlying vasculature from chronic topical steroid use. These cases feature the diverse presentations of skin atrophy on different Fitzpatrick skin types. Learning Points: Steroid atrophy is the most common side effect of chronic topical steroid use. Topical steroids are widely used for dermatologic conditions such as atopic dermatitis and plaque psoriasis. Steroids work to quell these inflammatory and autoimmune conditions and are overall tolerated well with proper use. Overuse of topical steroids is common and can cause known side effects of skin atrophy, erythema, striae, and telangiectasias. Recognition of steroid overuse requires knowledge of its presentation in various skin tones. In lighter skin types, atrophy is apparent with visible underlying vasculature and bright red erythema. In darker skin types, atrophy is more subtle and underlying vasculature may appear burgundy or maroon. Awareness of these differences in presentation will allow for quick recognition and immediate cessation of steroid use to prevent further side effects.
-

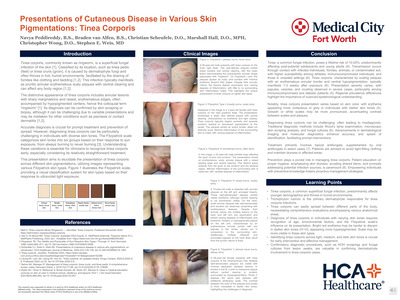
Presentations of Cutaneous Disease in Various Skin Pigmentations: Tinea Corporis
Navya Peddireddy, Braden van Alfen, Christian Scheufele, Marshall Hall, Christopher M. Wong, and Stephen Weis
Introduction: Tinea corporis, a superficial fungal skin infection, typically manifests as pruritic annular erythematous scaly plaques with central clearing. This condition can involve every body region. Here we present tinea corporis across various skin pigmentations. The goal of this presentation is to highlight distinctions and similarities in light, medium, and dark skin tones, using the Fitzpatrick scale for stratification of skin types. We hope this can aid primary care clinicians in early recognition of this common condition. Case Presentation: We present a series of cases illustrating the diverse manifestations of tinea corporis across different Fitzpatrick skin types. In Figure 2, a 28-year-old with Fitzpatrick I displays well-defined, scaly plaques on the inner thigh. Figure 3 features a 3-year-old of Fitzpatrick II with a large, poorly defined plaque on the right posterior thigh. A 33-year-old Fitzpatrick III male of showcases an erythematous, scaly plaque extending from the groin (Figure 4). Figure 5 presents a 15-year-old with Fitzpatrick IV, exhibiting well-demarcated erythematous plaques on the left arm with inflamed papules on the neck and arm. A 69-year-old female of Fitzpatrick V displays pink to violaceous plaques with hyperpigmentation and white/gray scales (Figure 6). These cases highlight the diverse clinical presentations that can be seen in different Fitzpatrick skin types. Learning Points: Tinea corporis is a common superficial fungal infection of the skin that tends to be more prevalent in younger demographics and thrives in humid environments. Trichophyton rubrum is the most common dermatophyte culprit for this fungal infection. It can spread easily between different parts of the body, accentuating the need for comprehensive skin examination encompassing all anatomical areas. Arriving at the correct diagnosis of tinea corporis across various skin tones involves recognizing the influence of age, prior and concomitant treatments, environmental factors, and the Fitzpatrick scale on its clinical presentation. Variations can be observed in the degree of scaling and the amount of erythema. Erythema is difficult to identify in darker Fitzpatrick skin types (IV-VI). Instead, erythema may appear hyperpigmentation. Likewise, scale may be more easily seen in these skin types. Identifying tinea corporis in light, medium, and dark skin tones is crucial for early intervention. Confirmatory diagnostic procedures, such as KOH scrapings and fungal cultures from lesion swabs are valuable in confirming the presence of dermatophyte involvement. If clinical suspicion remains high, a skin biopsy can be obtained for histologic confirmation.
-

Primary Resection of Duodenal Neuroendocrine Tumor with Suspected Lymph Node Metastasis: A Case Report
Raleigh Payton, David Bassa, Furrukh Jabbar, and Hassan Ahmed
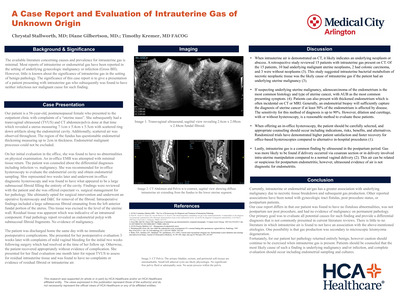
Introduction: Duodenal neuroendocrine carcinomas are an uncommon variant of Neuroendocrine tumors (NETs) that are typically non-functional with locoregional spread at the time of diagnosis. Management of these tumors is dependent on size, grade, stage, functional status and location.
Summary: A 66-year-old male presented with an incidental finding of low grade 3 centimeter duodenal NET on esophagogastroduodenoscopy (EGD) located in the second segment of the duodenum with evidence of lymphadenopathy on staging scans. In patients with suspected lymph node metastases, the first choice for curative intent is a pancreaticoduodenectomy (PD), also known as Whipple Procedure. We achieved surgical resection with free margins of the tumor via Robotic-assisted laparoscopic periampullary sparing duodenectomy with primary repair. In order to achieve preservation of the ampullary region, we identified the ampulla through transcystic duct guidewire insertion.
Case Presentation: A 66-year-old male presented for primary resection of duodenal NET following multiple EGD studies with attempted mucosal resection. He was scheduled for a robotic-assisted Whipple procedure. However at the time of the index operation, a primary resection of the tumor was completed with negative margins without performing the full procedure. Discussion Duodenal NETs often present in the first or second part of the duodenum. Subcentimeter non-ampullary locations are usually amenable to endoscopic resection. Periampullary NETs and duodenal NETs larger than 2 centimeters should be considered for surgical resection via local excision or PD. 20% of D-NETs occurring periampullary require complex procedures such as a PD. PD is the first choice for curative resection for suspected lymph node metastasis such as in our patient.
Conclusion: Primary resection of duodenal NETs can safely be removed robotically without performing life-altering Whipple procedures, even in cases of large tumor burden. These tumors must be located away from the ampullary region of D2, and precaution must be taken to preserve this area with primary closure. Lessons Learned: Preservation of the ampullary region can be achieved safely in robotic-assisted duodenectomy with use of a guidewire to ensure primary closure does not interfere with patency. Negative margins can be achieved safely even in the setting of a large duodenal tumor.
-

Quality Improvement Project: Compliance of Antenatal Testing in Patients with Class III Obesity
Isabella L. Sciacca, Timothy Kremer, and Nicole Tenzel
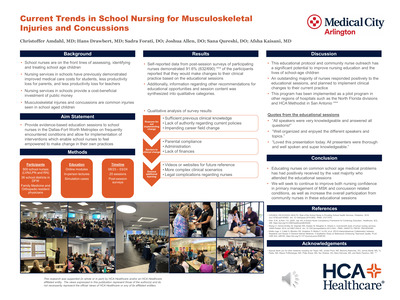
The prevalence of obesity in women of reproductive age (20 to 39) in the US is 39.7%. It has been estimated that one-quarter of pregnancy complications are attributable to maternal obesity. Comprehensive prenatal care is imperative to achieving positive health outcomes. This quality improvement (QI) initiative aimed to improve antenatal fetal surveillance rates in patients with class III obesity. Evidence based interventions to test fetal wellbeing were implemented and examined over a 7 month time period to evaluate physician compliance of the standard of care for antenatal surveillance starting at 34 weeks gestation. Following implementation of this initiative, compliance with weekly antenatal testing improved from an average of 30.0% to 91.4%. Strategies that contributed to the success of this project were frequent communication, team based workflow and active participation by physicians, staff and patients. Future implications include prevention of fetal and maternal complications of obesity.
-

Rare Rectal Lipoma Case Report
Victoria Nguyen, Sean Sojdie, Kunal Elete, Justin Richardson, and Long Hoang
INTRODUCTION: Colonic lipomas are rare, benign non-epithelial lesions of the gastrointestinal (GI) tract that predominantly affect elderly females and often found in the ascending colon. They are least common in the rectum, with a prevalence of 3.4%. Lipomas can grow to cause abdominal pain, bleeding, or obstruction. We report an incidental finding of a rectal lipoma in a patient presented with rectal bleeding. CASE: A 70 year-old male with a history of migraines presented to the hospital for two weeks of rectal bleeding and syncopal episode prior to arrival. Patient had visited the emergency department two weeks prior, but hemoglobin was 14.1 g/dL and vital signs were stable, so he was discharged home. Since then, he reported having four bowel movements daily with formed stools mixed with bright red blood. Notably, he uses two tablets of Excedrin daily for migraines. He denied dysphagia, abdominal pain, diarrhea, constipation, or melena. Labs showed a drop in hemoglobin from 14.1 to 9.3 g/dL. A CTA A/P revealed no active source of GI bleeding nor abnormal masses within the GI tract. Thus, it was decided to proceed with upper and lower endoscopies. Findings revealed H. pylori gastritis, sigmoid diverticulosis without active bleeding, and a polypoid lesion in the distal rectum with a positive pillow sign. Diagnosis was confirmed by Endoscopic ultrasound showing a rectal lipoma measuring 7 x 13 mm. No therapeutic intervention was deemed necessary. Upon discharge, rectal bleeding ceased, and hemoglobin stabilized. This case contributes to the broader understanding of this rare condition and its potential variations, ultimately aiding clinicians in making informed decisions when faced with similar cases in the future.
-

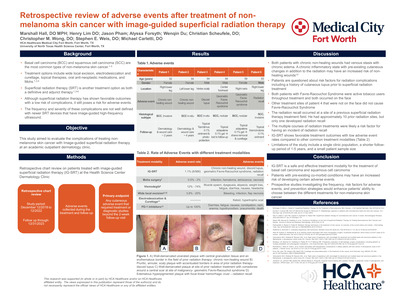
Retrospective Review of Adverse Events After Treatment of Non-Melanoma Skin Cancer with Image-Guided Superficial Radiation Therapy
Marshall Hall, Henry Lim, Jason Pham, Alyssa Forsyth, and Wenqin Du
-

Stop Horsing Around: A Case of Cenbuterol Toxicity
Justin Sanchez, Mark Cheneler, and Alexandra Villacres
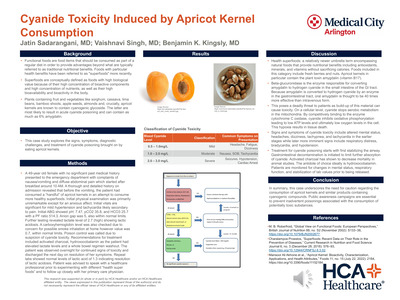
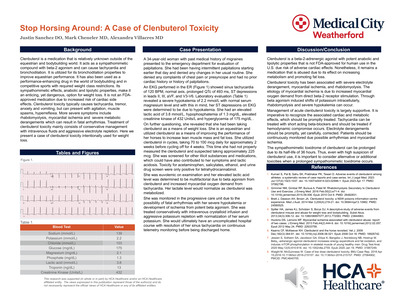
Introduction: Clenbuterol is a medication that is relatively unknown outside of the equestrian and bodybuilding worlds. It acts as a sympathomimetic compound with beta-2 agonism and can cause tachycardia and bronchodilation. It is utilized for this bronchodilation as a means of improving equestrian performance. Its sympathomimetic effects were utilized in the bodybuilding community as a weight loss medication by increasing catabolic metabolism. Here we present a case of intentional clenbuterol toxicity for weight loss. Case presentation: A 34-year-old woman with past medical history of migraines presented to the emergency department for evaluation of palpitations and an EKG showed sinus tachycardia of 120, normal axis, prolonged QTc of 493 ms, ST depressions in II, III, aVF, and V3-V6. Laboratory evaluation which show a serum potassium of 2.2 and her sinusoidal baseline was determined to be due to beer hypokalemia. She had access to clenbuterol from training horses and had utilized it as a weight loss medication cycling for 2 weeks of daily use in 4 weeks without. She had taken approximately 225 mcg and toxicology studies for acetaminophen, salicylates, ethanol, and urine drug screen were only positive for tetrahydrocannabinol. She was monitored in the progressive care unit with aggressive potassium replacement before being discharged after resolution of her sinus tachycardia. Discussion: Clenbuterol toxicity has been associated to myocardial ischemia and rhabdomyolysis. The etiology of myocardial ischemia is due to increased myocardial oxygen demand from unopposed beta agonism. The sympathomimetic toxidrome can be prolonged due to its half-life of 36 hours. Through beta agonism induced shifts of potassium intracellularly, rhabdomyolysis can occur. It is important to consider alternative toxicities when a prolonged sympathomimetic toxidrome occurs.
-

Stop That Bloody Cough: A Case of Hemoptysis After Intrapleural tPA Administration
Khizir Qureshi, Mark Cheneler, and Carlos Bahrami
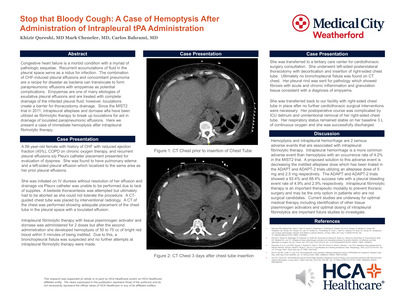
Introduction: Congestive heart failure is a morbid condition with a myriad of pathologic sequelae. Recurrent accumulations of fluid in the pleural space serve as a nidus for infection. The combination of CHF-induced pleural effusions and concomitant pneumonia are a recipe for disaster as bacteria can translocate to form parapneumonic effusions with empyemas as potential complications. Empyemas are one of many etiologies of exudative pleural effusions and are treated with complete drainage of the infected pleural fluid; however, loculations create a barrier for thoracostomy drainage. Since the MIST2 trial in 2011, intrapleural alteplase and dornase alfa have been utilized as fibrinolytic therapy to break up loculations for aid in drainage of loculated parapneumonic effusions. Here we present a case of immediate hemoptysis after intrapleural fibrinolytic therapy. Case presentation: A 56-year-old female with history of CHF, COPD, and recurrent pleural effusions s/p Pleurx catheter placement presented for evaluation of dyspnea and was found to have recurrent pleural effusion. Her effusion was initially managed with chest tube insertion but CT of the chest showed a loculated effusion and intrapleural fibrinolytic therapy was instilled. Immediately after her second dose, she had hemoptysis of 50 to 75 cc of bright red blood. She required transfer for cardiothoracic surgery with thoracotomy and decortication and was ultimately diagnosed with an empyema. Discussion: Hemoptysis and intrapleural hemorrhage are 2 serious adverse events that are associated with intrapleural fibrinolytic therapy. Intrapleural hemorrhage is a more common adverse event than hemoptysis with an occurrence rate of 4.2% in the MIST2 trial. A proposed solution to this adverse event is decreasing the instilled alteplase dose which has been trialed in the ADAPT and ADAPT-2 trials utilizing an alteplase dose of 5 mg and 2.5 mg respectively. The ADAPT and ADAPT-2 trials showed a 93.4% and 88.4% success rate with a pleural bleeding event rate of 4.9% and 2.9% respectively. Intrapleural fibrinolytic therapy is an important therapeutic modality to prevent thoracic surgery and may be the only option in patients who are not surgical candidates. Current studies for evaluation of other tissue plasminogen activators are underway and optimal medication and dosing of intrapleural fibrinolytics are important future studies to investigate.
-

Streptococcocal Induced Toxic Shock Syndrome: Importance of Diagnosis and Initiating Life Saving Treatment
Lincy Sakwa and Danielle Ford
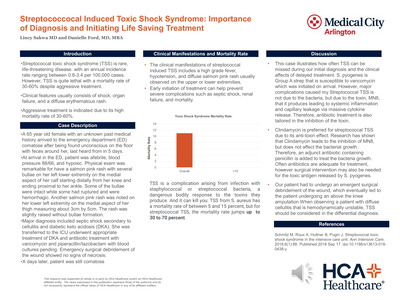
Toxic Shock Syndrome (TSS) is a toxin induced illness characterized by fever, rash, and hypotension. TSS low incidence report and rapid onset of clinical symptoms makes getting to the diagnosis critical so that treatment can be started as soon as possible. A 65-year-old woman was brought into the emergency department (ED) after being found on the floor unresponsive during a well fair check. It was noted that she has not been seen or heard from by her family members in the last five days. She has no known past medical history and she was unresponsive and hemodynamically unstable in the ED. She was afebrile, hypotensive with a blood pressure of 88/66, tachycardia, tachypneic, and hypoxemic with an oxygen saturation of 96% while on 5 liters of nasal cannula. On physical exam, patient was noted to have a salmon pink rash with several bullae on her left lower extremity on the medial aspect of her calf starting distally from her knee and ending proximal to her ankle. Some of the bullae was intact while some had ruptured and were hemorrhagic. Another salmon pink rash was noted on her lower left extremity on the medial aspect of her thigh measuring about 3cm by 5cm. The rash was slightly raised without bullae formation. Imaging done was negative for signs of osteomyelitis. Wound debridement of the lower left extremity of the medial calf showed no signs of necrotizing infections. At this time the diagnosis of septic shock due to cellulitis was made and the patient was started on vasopressors due to her hemodynamic instability. Antibiotic treatment with vancomycin and piperacillin/tazobactam was started for broad antibiotic treatment while blood and wound cultures were pending. However, as time went on, the patients’ hemodynamic status continued to deteriorate and was sent to the intensive care unit (ICU). While in the ICU blood cultures and wound cultures came back positive for Strep pyogenes. Strep pyogenes is Group A strep that are commonly treated with penicillin. The patient current antibiotic treatment was adequate for treatment, but surgical intervention was needed for the toxic antigen released by S. pyogenes. The patient had to undergo an emergent surgical debridement of the wound, which eventually led to the patient undergoing an above the knee amputation. After the surgical intervention and treatment of antibiotic, the patient recovered and was in stable condition.
-

Subacute Defibrillator Lead Associated Right Ventricular Perforation in a Young Individual with Non-Ischemic Cardiomyopathy: A Unique Clinical Case
Jackson V. Littlejohn, Aditya Sharma, Marisha R. Sharma, and Kamran Rizvi
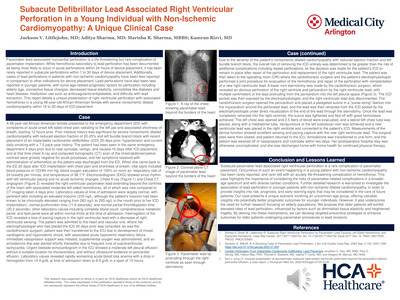
Pacemaker-lead associated complications are often documented in elderly populations with ischemic heart disease. Acute perforations within 24 hours of implantation are the most common, and immediate life-threatening complications are most likely to occur during an acute perforation. Subacute perforations between 1 day and 30 days after implantation are less common and carry a lower risk of life-threatening complications. Here, we present a unique case of subacute right ventricular perforation in a young individual with non-ischemic cardiomyopathy, challenging the conventional understanding of such an occurrence. Further adding to the intrigue of our case, the patient had recurrent hospital visits both before and after the perforation, allowing us to pinpoint the time of perforation a small window of 4 days, between postoperative day 16 and postoperative day 20. It also indicates a possibility that the near syncope, vertigo, and nausea experienced by the patient might be initial signs of impending perforation. This case highlights the importance of early recognition of possible pacemaker-lead perforation symptoms so that appropriate investigation and management may prevent further complications. While the younger age of the patient in this case might have a prognostic advantage, the possibility of right ventricular perforation in the setting of non-ischemic dilated cardiomyopathy requires further investigation to establish true association and risk.
-

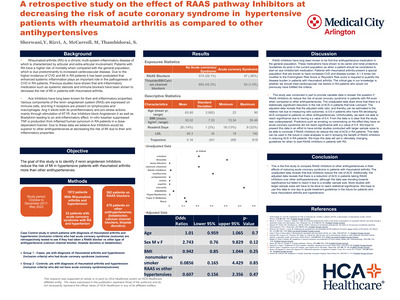
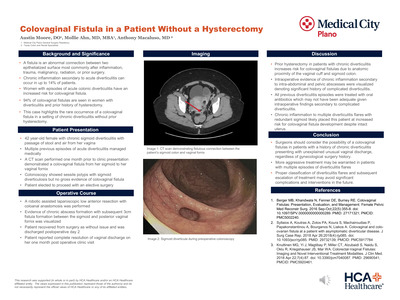
Surgical Margin Analysis in Early-Stage Cervical Cancer: An HCA Retrospective Study
Chrystal Stallworth, Abel Moron, Nicole Tenzel, Timothy Kremer, and Michele McCarroll
Objective: This study aimed to compare surgical margin analysis on final pathology in robotic assisted approach hysterectomy vs. all other approaches in early-stage cervical cancer.
Methods: Patients with clinical early-stage disease who underwent total and radical hysterectomy from the years 2018-2023 were categorized into robotic assisted approach group (RAH) vs all other approaches including laparoscopic hysterectomy (LAH), laparoscopic assisted vaginal hysterectomy (LAVH), and open hysterectomy (TAH). Fisher’s exact test was used for analysis of the primary outcome measure.
Results: A total of 92 patients met inclusion criteria. Mode of surgery included: 83 RAH (90.2%), 6 LAH (6.5%), 2 TAH (2.17%), and 1 LAVH (1.08%). Histologic subtypes included: 64 with squamous (69.56%), 27 with adenocarcinoma (29.34%), and 1 with adenosquamous (1.08%). A positive surgical margin status was found to have a significant association with the presence of LVSI (p=0.0002, RR= 30.0). The use of robotic assisted approach in total and radical hysterectomy for early-stage cervical cancer was not found to have a statistically significant association with surgical margin status (p=0.4707) when adjusted for uterine weight and length. No significant difference was observed in surgical margin status when adjusted for pathological stage (=0.0565, p=0.9721). Of the patients sampled, 58 were stage IA (63.04%), 31 were stage IB (33.69%), and 3 were stage II or III (3.26%) on final pathology. Positive margin status was observed in 6.02% of the robotic assisted group and 11.11% in the all other approaches group. Lymphovascular space invasion (LVSI) was observed at a lower rate (13.25 vs 22.2%) in the robotic assisted hysterectomy group. Radical hysterectomy was found to be attempted/completed at a higher rate in RAH vs all other approaches cohort (38.05% vs 22.22%).
Conclusion: The study demonstrated that surgical route and margins played a role only in LVSI patients.
-

Survival After Emergency Clamshell Thoracotomy with Bilateral Atrial Appendage Injuries
Jennifer Austin, Enrique Alvarez, Alicia Lay, and Christian Minshall
INTRODUCTION: The probability of survival is poor in patients who require a resuscitative thoracotomy, reported in the literature to be 9-20%. Outcomes are worse in patients who have suffered blunt trauma compared to penetrating trauma reported between 2-7%. Many studies have been done to evaluate clinical predictors of survival versus mortality. We present a case of high-mechanism blunt trauma with a high injury severity score of 34 who survived after an emergency clamshell thoracotomy with full neurological recovery.
CASE PRESENTATION: This case highlights a 28-year-old male who arrived as a transfer to a level 1 trauma center following high mechanism blunt trauma with known right hemothorax and aortic transection. Initial interventions were arterial line placement, cordis central venous catheter placement, and massive transfusion protocol (MTP) activation. After losing pulses in the trauma bay, he underwent ACLS, right thoracotomy with extension to clamshell thoracotomy and was taken to the operating room for exploration and control of hemorrhage. His injuries included Bilateral atrial appendage injuries cardiac tamponade secondary to bilateral atrial appendage injuries, aortic transection, T2-T4 vertebral body fractures, left ribs 2-7 and right ribs 2-5 fractures, right femoral head fracture, left acetabular rim fracture. He was discharged home on hospital day 30 neurologically intact.
LEARNING POINTS: The credit to his survival is multifactorial. He arrived at a level 1 trauma center with the capability for massive transfusion, which was able to give him a total of 90 units of blood products. Supplies were immediately available when needed. The nursing and support staff in the trauma bay were well-trained and performed their duties at the highest level of expectation. Furthermore, the collaboration between the ED physicians, RNs, support staff and the trauma team led to expeditious care without undue delays. Being prepared for a broad array of injuries in the trauma bay is paramount to a quick and efficient resuscitation. This includes having equipment (invasive lines, chest tubes, a rapid transfuser, and thoracotomy instruments) and ancillary staff (blood bank, radiology, and operating room) readily available as well as emergency room staff who are trained and proficient in techniques and procedures that may be required. Perhaps often overlooked, the collaboration between the ER staff, the EM physicians and the trauma team also contributes to a smooth, seamless resuscitation.
-

Systemic Storm: Multi-Organ Septic Emboli in Acute Aortic Valve Endocarditis
Jilpa Shah, Akshaj Pole, and Amnah Andrabi
According to the Infectious Disease Society of America (IDSA), Infective endocarditis (IE) is an infection of the endocardial surface of the native valve, prosthetic heart valve, or an implanted cardiac device such as a permanent pacemaker or a defibrillator. IE is a rare fatal disease with an incidence rate of 3 to 10 cases per 100,000 people, predominantly in males over the age of 50 years in developed countries. Septic emboli are a serious sequelae of infective endocarditis with commonly affecting brain, spleen, kidneys, and lung. Usually, initial management includes tapered long term antibiotics with surgical evaluation for possible valve replacement. Here, we present the case of an 80 year old male with no significant past medical history or known valvular abnormalities, who came in with generalized weakness and right sided abdominal pain. Patient was initially admitted for sepsis secondary to UTI and right sided hydroureteronephrosis. Blood and urine cultures were positive for Staphylococcus aureus, and Transthoracic echocardiogram revealed medium size vegetation on the aortic valve, thus, confirming the diagnosis of acute aortic valve infective endocarditis. Clinical course evolved into multiple septic emboli to nearly all vascular territories in the brain, splenic infarct, and acute limb ischemia. Unfortunately, the significant clot burden led to rapid clinical deterioration and ultimate demise of the patient. A brief literature search suggests the rarity of superimposed complications of IE in a single patient without significant risk factors. Early recognition and prompt surgical intervention is vital toward improving outcomes in patients with IE as perioperative risk can increase exponentially when delays arise in management.
-
 at Weatherford by Feeza Hasan, Diana Steedley, Maria Guerrero, and Muhammad Siddique")
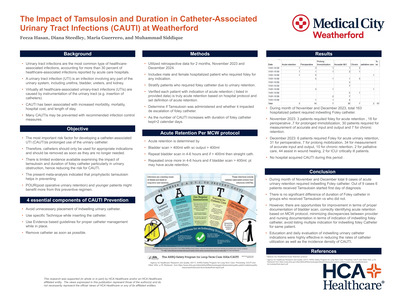
The Impact of Tamsulosin and Duration in Catheter-associated UTI (CAUTI) at Weatherford
Feeza Hasan, Diana Steedley, Maria Guerrero, and Muhammad Siddique
Among Catheter-Associated Urinary Tract Infections (CAUTI) acquired in the hospital, approximately 75% are associated with a urinary catheter, which is a tube inserted into the bladder through the urethra to drain urine. Between 15-25% of hospitalized patients receive urinary catheters during their hospital stay. A urinary tract infection (UTI) is an infection involving any part of the urinary system, including urethra, bladder, ureters, and kidney. UTIs are the most common type of healthcare-associated infection reported to the National Healthcare Safety Network (NHSN). The most important risk factor for developing a CAUTI is prolonged use of the urinary catheter. Therefore, catheters should only be used for appropriate indications and should be removed as soon as they are no longer needed. Tamsulosin is a selective alpha1A-adrenergic receptor antagonist. The effects of tamsulosin are targeted for the smooth muscle receptors of the prostate and urethra. Blocking this receptor relaxes the smooth muscle of the bladder and urethra to improve urine flow. There is limited evidence available examining the impact of tamsulosin and duration of foley catheter particularly in urinary obstruction, hence reducing the risk for CAUTI. The present meta-analysis indicated that prophylactic tamsulosin helps in preventing POUR (post-operative urinary retention) and younger patients might benefit more from this preventive regimen. Our goal is to utilize retrospective data for last 2-3 months and include the patient with CAUTI who were on foley catheter due to urinary retention. We excluded patients with urinary retention due to other cause and post-operative patient on foley catheter. then determine when Tamsulosin was administered and whether it impact de-escalation of foley catheter. As the number of CAUTI increases with duration of foley catheter kept>2 calendar days. During month of November and December 2023, total 163 hospitalized patient required indwelling Foley catheter. November 2023: 3 patients requited foley for acute retention , 18 for perioperative ,7 for prolonged immobilization, 30 patients required for measurement of accurate and input and output and 7 for chronic retention. December 2023: 6 patients required Foley for acute urinary retention, 31 for perioperative, 7 for prolong mobilization, 34 for measurement of accurate input and output, 10 for chronic retention, 2 for palliative care, 44 assist in wound healing, 2 for ICU/ critically ill patients. No hospital acquired CAUTI during this period. Education and daily evaluation of indwelling urinary catheter indications were highly effective in reducing the rates of catheter utilization as well as the incidence density of CAUTI.
-

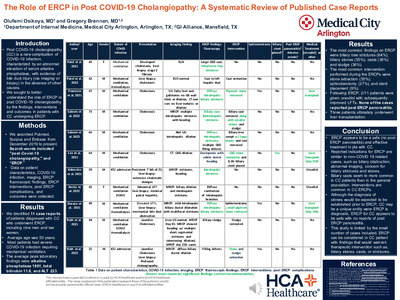
The Role of ERCP in Post Covid-19 Cholangiopathy: A Systemic Review of Published Case Reports
Olufemi Osikoya and Gregory Brennan
Introduction: Post COVID-19 cholangiopathy (CC) is a rare complication of COVID-19 infection. It is characterized by abnormal elevation of serum alkaline phosphatase, with evidence of bile duct injury (via imaging or biopsy) in the absence of other causes. Not much is known regarding the role of ERCP in post COVID-19 cholangiopathy. We sought to better understand the findings, interventions and outcomes in patients with CC undergoing ERCP. Methods: We searched Pubmed, Scopus and Embase from December 2019 to present. Search words included "post-Covid-19 cholangiopathy," and “ERCP.” Data on patient characteristics, COVID-19 infection, imaging, ERCP fluoroscopic findings, ERCP interventions, post ERCP complications, and outcomes were collected. Results: We identified 11 case reports of patients diagnosed with CC who underwent ERCP, including nine men and two women. The average age was 50 years. Most patients had severe COVID-19 infection requiring mechanical ventilation. The average peak laboratories were alkaline phosphatase 1601, total bilirubin 11.8, and ALT 223. The most common findings on ERCP were biliary tree strictures (64%), biliary stones (55%), casts (36%) and sludge (36%). The most common intervention performed during the ERCPs were stone extraction (55%), sphincterotomy (27%), and stent placement (9%). Following ERCP, two of the 11 patients were given ursodiol with subsequently improved LFTs. None of the cases reported post ERCP pancreatitis. Two patients ultimately underwent liver transplantation. Discussion: In patients with CC, ERCP appears to be a safe and effective treatment. Reported indications for ERCP are similar to non-COVID 19 related cases, such as biliary obstruction, abnormal imaging, concern for biliary strictures and stones. The most common findings during ERCP in CC are strictures, stones, and biliary casts. Finding common bile duct stones does not rule out CC. Biliary casts seem to more common in CC patients than in the general population. Interventions are common in CC ERCPs. The most common intervention performed was stone or cast extraction. Although the diagnosis would be expected to be established prior to ERCP, CC may be a unique entity were ERCP is diagnostic. ERCP for CC appears to be safe with no reports of post ERCP pancreatitis. This study is limited by the small number of cases included. ERCP can be considered in CC patient with findings that would warrant therapeutic intervention such as, biliary stones, casts, or strictures.
-

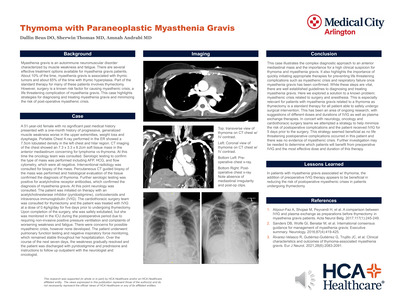
Thymoma with Paraneoplastic Myasthenia Gravis
Dallin Beus, Sherwin Thomas, and Amnah Andrabi
Background: Myasthenia gravis is an autoimmune neuromuscular disorder characterized by muscle weakness and fatigue. Paraneoplastic myasthenia gravis, a rare manifestation of this condition, is often associated with underlying malignancies, such as thymic tumors. We present the case of a 51-year-old female patient with a mediastinal mass who developed paraneoplastic myasthenia gravis, highlighting the diagnostic challenges and therapeutic considerations in such cases. Case Description: A 51-year-old female presented with a one-month history of progressive muscle weakness, diplopia, and dysphagia. Clinical examination and serological tests led to the diagnosis of myasthenia gravis. Computed tomography (CT) imaging revealed a 6 cm mediastinal mass, suggestive of a thymic tumor. Further workup, including histopathological examination, confirmed a thymic carcinoma as the underlying malignancy. This case highlights the complex interplay between thymic tumors and myasthenia gravis, suggesting a paraneoplastic origin. Treatment and Outcome: The patient was initiated on treatment with acetylcholinesterase inhibitors and corticosteroids for myasthenia gravis, with concurrent intravenous immunoglobulin (IVIG) therapy. Subsequently, she underwent a thymectomy, and adjuvant chemotherapy was administered for the thymic carcinoma. The patient's recovery was uneventful, with no postoperative myasthenic crisis observed. Over time, her muscle strength improved, and she achieved symptomatic remission of myasthenia gravis. Regular follow-up revealed no evidence of tumor recurrence, and the patient remained free of myasthenia gravis-related symptoms. Conclusion: This case report highlights the importance of considering paraneoplastic myasthenia gravis in patients with mediastinal masses, especially thymic tumors. Prompt diagnosis and multimodal treatment, including thymectomy, IVIG therapy, and oncological therapy, are crucial in managing these complex cases. Timely recognition and intervention are pivotal in achieving favorable clinical outcomes for patients with this rare and challenging association. The addition of IVIG therapy appears to be beneficial in reducing the risk of postoperative myasthenic crises in these patients.
-

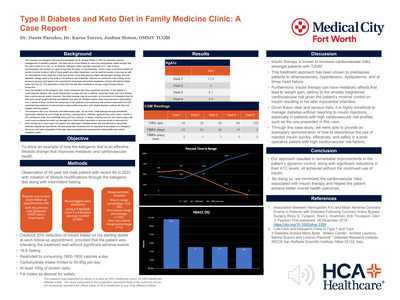
Type II Diabetes and Keto Diet in Family Medicine Clinic: A Case Report
Dante Paredes, Karos Torres, and Joshua Moton
The management of patients with high cardiac risk profiles who require insulin therapy for diabetes can be challenging due to the potential adverse effects of insulin on cardiovascular health. In order to achieve remission of type 2 diabetes mellitus (T2DM) and discontinue the need for insulin, weight loss has long been recognized as a valuable approach. The goal for this case was to implement dietary and lifestyle changes in a safe and efficient manner to induce remission of T2DM, without increasing the sympathetic load often associated with fully dosed ketogenic and other fasting strategies. This case report highlights the successful management of a 40-year-old male patient with high cardiac risk factors and a history of untreated T2DM who required insulin therapy. After experiencing a ST elevation myocardial infarction (STEMI) and subsequent three vessel coronary artery bypass graft (CABG), the patient was found to have an A1C of 11.6% and a BMI of 31.5 kg/m2. A comprehensive treatment approach was employed, which included carb restriction, intermittent fasting (IF), a ketogenic diet (KD), and non-insulin medications to gradually wean the patient off insulin therapy. With regular follow-ups with his primary care physician (PCP) and strict adherence to the treatment plan, the patient achieved remarkable results. After three months of treatment, the patient's A1C dropped to 5% and BMI decreased to 27.3 kg/m2, enabling discontinuation of insulin use. The patient remained in remission throughout repeated follow-ups over the next 6 months while maintaining dietary and exercise habits, as well as continuing his other medications, including Metformin. This case underscores the potential effectiveness of a low-calorie ketogenic diet with exercise as a valuable tool for acquiring and maintaining remission of T2DM in patients with obesity and high cardiac risk factors.
-

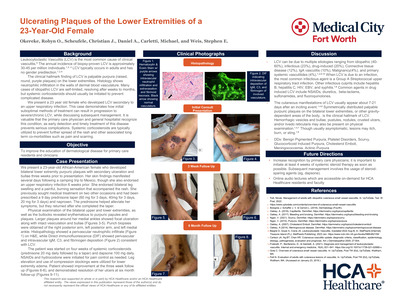
Ulcerating Plaques of the Lower Extremities of a 23-Year-Old Female
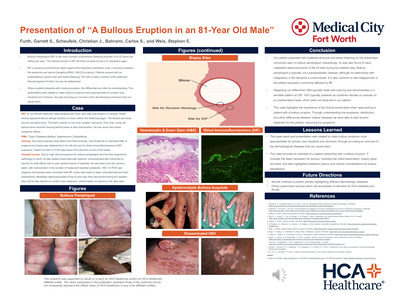
Robyn O. Okereke, Christian J. Scheufele, Michael Carletti, Stephen E. Weis, and Carlos Bahrami
INTRODUCTION: What should come to mind when any physician sees dark red spots on the legs? If you answered vasculitis, then you are on the right track. Leukocytoclastic vasculitis (LCV) is defined as small vessel inflammation of the dermal capillaries and venules. The clinical hallmark finding of LCV is palpable purpura (raised, round, purple plaques) on the lower extremities. LCV is confirmed by histopathology showing neutrophilic infiltration in the walls of dermal vasculature. Though LCV is the most common cause of clinical vasculitis, the annual incidence of biopsy-proven LCV is approximately 30-45 per million individuals. LCV typically occurs in adults and has no gender predilection. Though idiopathic 60% of the time, LCV may be secondary to other causes, including infection, drugs, systemic disease, or malignancy. CASE PRESENTATION: We present a 23-year-old African-American female who developed bilateral lower extremity purpuric plaques with secondary ulceration and bullae three weeks prior to presentation. Her skin findings manifested several days following a camping trip to Mexico, though she also endorsed an upper respiratory infection 6 weeks prior. She previously sought medical treatment on two other occasions and had been prescribed a 9 day prednisone taper and naproxen. The prednisone helped alleviate her symptoms, but they returned after she completed the taper. Biopsies were obtained with histopathology showing a perivascular neutrophilic infiltrate consistent with LCV. The patient was started on four weeks of systemic corticosteroids (prednisone 20 mg daily followed by a taper) and dapsone 100 mg daily. NSAIDs and hydrocodone were initiated for pain control as needed. Leg elevation and use of compression stockings were utilized for lower extremity edema. Patient showed improvement at the three week follow up, and demonstrated resolution of her ulcers at six-month follow-up. LEARNING POINTS: Many cases of LCV are self-limited and resolve after weeks to months. Treatment depends on etiology and disease severity. This case demonstrates how initial suboptimal treatments can result in progression to severe/chronic LCV. In patients with chronic disease duration and/or complicated physical exam findings (eg, ulceration/bullae), it is important to initiate at least 4 weeks of systemic steroid therapy as soon as possible. Subsequent management involves the usage of steroid-sparing agents (eg, dapsone). It is valuable that the primary care physician and general hospitalist recognize this condition, as early detection and timely treatment prevents serious complications.
-

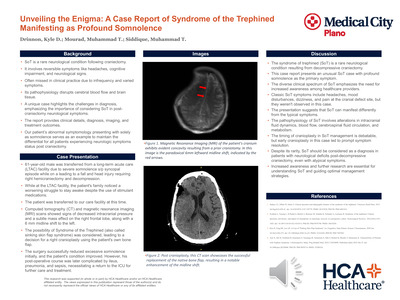
Unveiling the Enigma: A Case Report of Syndrome of the Trephined Manifesting as Profound Somnolence
Kyle Drinnon, Muhammad T. Mourad, and Muhammad Siddique
The Syndrome of Trephined (SoT), also known as, "sinking skin flap syndrome," is a rare neurological complication that can occur after craniectomy. It can manifest with various reversible neurological symptoms such as headaches, mood changes, cognitive impairment, and focal neurological signs. The underlying pathophysiology of SoT is not completely understood but is believed to result from changes in intracranial and cerebrospinal fluid dynamics due to the loss of the protective cranial enclosure following craniectomy. Despite its rarity, healthcare providers should consider SoT as a possible diagnosis in patients who develop neurological deficits after undergoing decompressive craniectomy, even if their symptoms are unusual. In this case, we describe a 61-year-old male who presented with excessive somnolence following a right hemicraniectomy after a head strike with a resulting frontal hematoma and subarachnoid hemorrhage. Imaging evaluation revealed reduced intracranial pressure and a subtle mass effect on the right frontal lobe, resulting in a 6 mm midline shift to the left. After undergoing cranioplasty, the patient's neurological status markedly improved. Our case underscores the importance of recognizing the diverse manifestations of SoT for prompt diagnosis and management. Additionally, it highlights the potential advantages of early cranioplasty in improving neurological symptoms.