


-

Impact of MIPS Measure 66 on the Incidence of PTA's
Sydney Finch and Christopher Houston
INTRO
A number of randomized controlled trials indicate that using point-of-care group A strep (POC GAS) testing decreases antibiotic utilization without compromising health outcomes. In 2018, the Merit-based Incentive Payment System (MIPS) measure 66 went into effect requiring the testing for GAS when treating pharyngitis. The intent was to decrease the unnecessary use of antibiotics in the treatment of pharyngitis, given that most cases are viral. Anecdotally, some physicians have noticed the increased incidence of peritonsillar abscesses (PTA). Our research group aims to investigate if there has been a significant increase in incidence of PTAs after the implementation of MIPS measure 66.
METHODS
We chose two different study periods to compare the incidence of PTAs. 2017 was the last year before MIPS measure 66 was implemented. We chose to compare to 2019. We felt this was appropriate because it gave providers 1 year for the changes to be fully adopted and before seasonal infectious disease radically changed in early 2020 due to the COVID 19 pandemic. During 2017, ICD9 codes were used. 2019 utilized ICD 10 codes. The following diagnoses related to PTAs were used: Peritonsillar (tonsillar) abscess, parapharyngeal abscess, retropharyngeal abscess, and other abscesses of pharynx.
RESULTS
We first obtained feasibility data from the enterprise data warehouse. From 1/1/2017 through 12/31/2017, there were 3342 patients enterprise wide with the diagnosis codes related to PTA. From 1/1/2019 - 12/31/2019, there were 4006 patients with a diagnosis related to PTA. This indicated that there are enough patients to proceed to see if there is a statistically significant difference in the incidence before and after the implementation of MIPS measure 66. We plan to normalize the data with respect to the number of patients in the same time periods presenting to the ED with sore throat related chief complaints for final analysis.
CONCLUSION
Prior studies show that use of POC GAS testing decreases the antibiotic utilization, and MIPS measure 66 mandates the use of this testing. The absolute number of cases of PTA related diagnoses did increase after the implementation of MIPS measure 66. We will proceed to determine if the incidence with respect to patients presenting with sore throat related chief complaints changed after the implementation. The results of this comparison may warrant changes in empiric antibiotic coverage in certain cases of pharyngitis.
-

Implementation of Standardized Screening and Patient Education Regarding HPV Vaccination Within an OB-GYN Clinic
Kristina Krupa and Nicole Tenzel
Background: Each year, millions of women become infected with Human Papillomavirus Virus (HPV). The HPV virus can cause multiple types of cancer including cervical, vaginal, vulvar, penile, anal, vaginal, and oropharyngeal. HPV vaccination has the potential to prevent majority of these cancers. Despite this, a large portion of the United States population remains unvaccinated. Standardizing screening protocols and patient education materials within our OBGYN clinic can help educate patients about the HPV vaccine benefits and facilitate shared decision-making regarding vaccination.
Methods: This ongoing quality improvement project was initially created as a single-phase initiative that involved implementation of a screening questionnaire regarding HPV vaccination status and a standardized informational HPV flyer given to patients without history of vaccination. The screening questionnaire and flyer were to be given to all patients within the eligible age range of vaccination at well women exams, new patient gynecologic visits, and 4-6 week postpartum visits.
Review of the data collected identified opportunities for process improvement; thus, a second phase of the project is currently ongoing. Phase two involves physician initiation of conversation regarding HPV vaccination history at all well women exams, providing the standardized HPV informational flyers, and allowing for shared decision-making regarding HPV vaccination.
Results: The first phase of the project revealed 37.2% of eligible patients were screened for vaccination history and given an HPV informational flyer if applicable. Data collection for the second phase of the project with process improvements is ongoing.
Conclusion: This ongoing quality improvement project aims to standardize screening for HPV vaccination history and provide patient education regarding HPV vaccination for eligible patients within our OBGYN clinic. Ongoing evaluation of the workflow process will help us to implement the most feasible strategy to sustain screening and patient education regarding HPV vaccination, ideally increasing vaccination rates among our patient population to decrease HPV related cancers.
-

Improving Cord Gas Collection Rates on Labor & Delivery
Sandra Zhi, Diane Gilbertson, Ifeoluwa Adesina-Aina, Sarah Moore, and Jack Graham
Background: Cord blood gas measurements are helpful to determine the acid-base status of a neonate after delivery and can determine risk for neonatal encephalopathy. Collection usually occurs right after delivery of the infant and after the umbilical cord has been cut and clamped. The OBGYN residents are currently trained to draw cord blood for gas analysis if clinical status of the neonate is subpar, but there exist other indications for drawing cord blood to send for cord gases as recommended by the American College of Obstetricians and Gynecologists as well as the American Academy of Pediatrics. This project will focus on educating residents in the various indications for collecting cord gases and encouraging a higher rate of collection in order to assess fetal condition at the time of delivery.
Methods: The Graduate Medical Education office patients who delivered in the month of September 2025 will be reviewed and the percent of patients with a cord gas analysis collected at the time of delivery will be noted. It is expected that this percentage is very low given that there exists no standard with collecting cord gases unless the neonate’s clinical status is concerning as determined by APGAR scores. Then, the project team will present a list of indications for which cord gas collection is encouraged to the residents at their weekly Didactics. The team will also continue to remind the residents with email notification. Then, the Graduate Medical Education deliveries that occur between November 2025 - January 2026 will be reviewed and the rate of collection will be obtained for that period of time. These two rates will be compared and conclusions will be drawn about how to establish a new internal standard of care.
Results: We do not have any formal results currently as we are in the data collection process but will be able to present results by the North Texas Research Forum date. Conclusions: We do not have any formal results currently as we are in the data collection process but will be able to present results by the North Texas Research Forum date.
-

Improving the Utilization of Palliative Care Services at Medical City Fort Worth
Gennipher Smith, Shervin Sarji, Maanasa Palani, Samuel Chen, Mary Halm, Kristina Bowman, and Morvarid Rezaie
Palliative Care (PC) is a specialized medical care that aims to optimize the quality of life and alleviate the suffering of patients with serious medical illness. Benefits of palliative care include improved symptom management, enhanced quality of life, reduced healthcare utilization, better care alignment, improved communication and support, and financial savings. Hospital Corporation of America (HCA) Medical City Fort Worth (MCFW) has a PC consult service. However, it is underutilized. According to data collected from January 2025 to December 2025, the percentage of PC consults for high risk units, such as oncology and ICU, by day 3 of admission varies by unit and fluctuates from month to month. We aim to perform a quality improvement project at MCFW to improve the use of PC services. Utilizing literature reviews, gathering feedback from the PC nurses, and analyzing statistical data from the PC team, we plan to develop learning resources that will enhance the understanding of the benefits of PC as a part of the care team for people with serious, chronic, or life-limiting illnesses. Our goals are to increase the amount of PC consults 3% by 12/31/2026 and increase PC screening by nurses 2% by 12/31/2026. Potential methods to improve PC consults include posting a PC visual aid in physician dictation rooms, peer-to-peer quarterly PC presentations to residents, and an easy access resident physician narrated PC PowerPoint. We will evaluate the quantity of PC consults that are placed in 2026 and determine if these methods are effective in accomplishing the goals. We will also evaluate additional areas of improvement that will continue to enhance utilization if our changes are not effective or sufficient.
-

Improving Trauma Resuscitation Through Video Review: A Quality Improvement-Oriented Literature Review
Joshua Smith and Leena Iqbal
Background Trauma resuscitation is a high-acuity, time-critical environment characterized by diagnostic uncertainty, simultaneous interventions, and complex team dynamics. Despite the widespread adoption of standardized trauma frameworks such as Advanced Trauma Life Support (ATLS), deviations from best practice and process variability remain common. Trauma video review (TVR) has emerged as a method to objectively evaluate resuscitation performance beyond traditional documentation.
Methods A narrative literature review was conducted of English-language publications examining the use of video recording and structured video review in trauma resuscitation. Peer-reviewed articles and relevant gray literature were identified through database and citation searches. Included works evaluated TVR for assessment of clinical processes, protocol adherence, team performance, and educational outcomes. Studies focused solely on technical recording systems without clinical application were excluded. Findings were synthesized thematically.
Results The reviewed literature demonstrates that TVR enables more precise and objective assessment of trauma resuscitation than chart review alone. Reported benefits include improved measurement of time-dependent interventions, identification of latent process failures, enhanced evaluation of team communication and role clarity, and targeted educational feedback. TVR was consistently described as valuable for assessing both technical and non-technical skills. Common barriers to implementation included medicolegal concerns, privacy and data governance challenges, resource requirements, and cultural resistance related to perceived surveillance.
Conclusion Trauma video review is well supported in the literature as a powerful tool for objective evaluation of trauma resuscitation performance and team dynamics. Its successful adoption depends on careful attention to legal, ethical, technical, and cultural considerations to ensure its use as a learning and improvement modality rather than a punitive mechanism.
-

Induced Vaginal Delivery in Pregnant Patient with Enlarging Choroidal Hemangioma
Sandra Zhi, Allison Burkes, Monica Saripella, Bhagyashri Pandey, Keith Storts, Kishan Patel, and J William Harbour
INTRODUCTION: Sturge Weber Syndrome (SWS) is a rare congenital neurocutaneous disorder affecting capillary formation, classically presenting with a facial port-wine birthmark and seizures. Associated symptoms vary by individual but may include additional brain and eye manifestations such as cognitive impairment, headache, stroke-like episodes, and glaucoma or visual field defects. Because SWS results from a sporadic mutation, it does not carry specific contraindications to pregnancy regarding fetal risk. However, pregnancies in patients with SWS should be managed by an multidisciplinary team and closely monitored for acute neurological and ophthalmologic complications. In childbirth, previous case reports have favored Cesarean section over vaginal delivery to minimize increases in intracranial pressure on abnormal cerebral or ocular capillaries, potentially worsening vision.
CASE SUMMARY: Here, we present a 21-year-old primigravid woman with known SWS who received routine antepartum care in our OBGYN clinic. At 32 weeks gestation, she was found to have a new serous retinal detachment and an enlarging choroidal hemangioma in her only seeing eye, placing her at high risk for rapid, irreversible vision loss. Given the worsening detachment and her progressive visual symptoms, a multidisciplinary team involving Maternal–Fetal Medicine, Retina, and Ocular Oncology recommended emergent induction of labor at 34 weeks and 3 days to allow expedited postpartum ophthalmologic treatment. She progressed quickly during induction, with a five-minute second stage, and delivered a healthy but premature infant without complications. Outside of her ophthalmologic disease, her pregnancy remained uncomplicated. She was discharged on postpartum day one to attend same-day ophthalmology follow-up to plan radiation treatment not feasible during pregnancy.
CONCLUSION: Progressive choroidal hemangioma in pregnancy is uncommon and poorly described, and vaginal delivery has not yet been utilized as seen in the literature for these patients. Thus, patients with SWS and concurrent ocular pathology require coordinated care involving obstetrics, ophthalmology, and subspecialty teams. This case illustrates that vaginal delivery can be a safe and appropriate option for pregnant patients with vision-threatening retinal detachment and choroidal hemangioma when supported by close multidisciplinary management. This case also supports the potential role of propranolol as an adjunctive agent in reducing labor duration, consistent with reports suggesting it may shorten the second stage of labor.
-

Inpatient Dermatology: Dermatology Consults at Medical City Fort Worth
Olivia Gruver, Marshall Hall, Henry Lim, Christina Guo, Garrett Furth, Stephen E. Weis, Dustin Wilkes, and Michael Carletti
Background: Inpatient dermatology is an important yet evolving field. There has been a linear decrease in the number of dermatologists providing inpatient care and in the number of medical centers with an inpatient dermatology service. Medical centers with inpatient dermatology services are unevenly distributed geographically, with most in larger metropolitan areas. There is still a great need for dermatologic expertise in the inpatient setting. We aim to examine the utility of the dermatologic consult service, including the most common chief complaints and conditions that prompted consultation over four months at Medical City Fort Worth.
Methods: This was a retrospective chart review study investigating consultations to the dermatology service at Medical City Fort Worth hospital between September 1, 2025, and January 8, 2026. Patient clinical diagnoses were reviewed.
Results: There were 27 dermatology consults. The internal medicine service requested all consultations. All consultations were done on admitted patients; however, three consults were seen in the ED. Of the 27 patient consultations, 13 (48%) were admitted for a primary dermatologic complaint. 19 patients had a biopsy performed (70%) for disease confirmation. 18 consults had a chief complaint of rashes (67%), followed by 5 for wounds (22%) and 3 for nonhealing lesions (11%). The most frequently diagnosed dermatologic conditions were infectious (22%) and inflammatory (22%), followed by malignancies (18%) and drug eruptions (14.8%).
Conclusions: Inpatient dermatology consultations are a valuable resource to the inpatient team, especially when the primary diagnosis is a dermatologic condition. Biopsies help confirm the diagnosis and management of dermatologic conditions presenting in the inpatient hospital setting.
-

Integration of AI Resources to Enhance Obstetric and Gynecology Resident Education
Victoria Ruggiero, Cameron Stokes, and Nicole Tenzel
Background: Graduate medical education faculty, while responsible for overseeing the clinical training of their residents, are additionally tasked with providing effective resident education. AI offers a potential solution to enhance development and delivery of educational topics to their trainees, while decreasing the time needed to prepare formal education resources. This study aims to evaluate resident satisfaction for different learning tools generated by AI platforms while also assess their retention of clinical content.
Methods: Three topics related to menopause were identified: (1) Menopause Physiology and Diagnosis, (2) Hormonal Therapy for Treatment of Vasomotor Symptoms, and (3) Treatment of Genitourinary symptoms. Evidence-based resources (UpToDate) were selected for each of these topics and introduced into the following AI resource generators – Gamma (PowerPoint generator), Revisely (Flashcard generator), and NotebookLM (Podcast generator). Medical City Arlington OBGYN residents will be divided into three groups. Each group will be assigned different AI-generated content as it relates to each menopause topic (e.g. Group 1 – Menopause Physiology and diagnosis: flashcards, hormonal therapy for treatment of vasomotor symptoms: podcast, treatment of genitourinary symptoms: PowerPoint). After utilizing each tool, the residents will complete a 10-question quiz looking at information retention, as well as a survey to assess learner preference and engagement. These evaluations will allow for an objective measure of teaching effectiveness as well as collecting information on user experience and feedback.
Results/Conclusion: This project is planned to be implemented in February 2026. It is anticipated that results gathered from both the quizzes and survey will show that AI-generated resources are effective tools for content delivery in medical education. Additionally, it is predicted that residents will express that incorporation of AI-generated resources are beneficial and identified by learners that these are valuable tools to incorporate into their training.
-
 Multicenter Registry by April Miller, Pranay Arora, Devika Pavuluri, and John Bini")
Internal Jugular Injuries: Outcomes from the American Association for the Surgery of Trauma PROspective Observational Vascular Injury Treatment (PROOVIT) Multicenter Registry
April Miller, Pranay Arora, Devika Pavuluri, and John Bini
Introduction: Since March 2013, the PROOVIT database has been a prospective, multi-center observational trial established for the study of vascular trauma. Here we present the data for the management of internal jugular vein injuries due to blunt and penetrating trauma.
Methods: Inclusion criteria for the PROOVIT study included patients age >2 years with radiologic or clinical/operative diagnosis of injury to named vessels in trauma patients at participating facilities. The database was reviewed to examine injury presentation, surgical management, postprocedural medical management with antiplatelet or anticoagulant therapy, and mortality. SPSS software was used to perform the descriptive and exploratory analysis for the study sample dataset.
Results: Ninety-four injuries were reported over a 10-year period beginning in 2013 from 21 Level 1 and one Level 2 trauma centers. Ten were blunt, 83 penetrating, and 1 mixed blunt/penetrating with 45 transected, 8 occluded, 3 pseudoaneurysm, and 26 injuries with partial transection or flow limiting defect. Seventy-five patients underwent operative exploration - 49 being ligated, 1 endovascular repair, and 39 primary repair. Anticoagulation (AC) included 4 patients on IV heparin, 19 on LMWH, and 1 on apixaban. Six were discharged on AC and 19 on anti-platelet medications. In-hospital mortality was 18% of the 94 total patients, excluding 2 with unreported outcomes. Based on the binomial regression analysis, higher ISS score, lactate, and PRBC transfusion requirements were associated with increased risk of in-hospital mortality (8.3%, 12.5%, and 20.4% respectively). Normal hemoglobin was associated with decreased risk of in-hospital mortality. P-values for independent variables of type of injury, repair vs ligation, ISS score, blood lactate, number of PRBC transfusions, hemoglobin level, and type of primary repair exceed the 0.05 significant threshold. This lack of statistical significance may be attributable to the small sample size.
Discussion: In review of IJV necessitating intervention, the majority were ligated. Nearly half were managed with primary repair, including thirteen with end-to-end anastomosis.
-
 Analgesia Medication Administration in Orthopaedic Surgery: A Brief Review by Jenna Chrabolowski, Troy B. Puga, Abanoub Attallahm, McKenna W. Box, and John T. Riehl")
Intraosseous (IO) Analgesia Medication Administration in Orthopaedic Surgery: A Brief Review
Jenna Chrabolowski, Troy B. Puga, Abanoub Attallahm, McKenna W. Box, and John T. Riehl
Introduction
Intraosseous (IO) analgesia is a novel strategy for pain control in orthopaedic surgery. This brief review aims to provide an overview of IO analgesia in orthopaedic surgery.
Methods
A search was conducted across seven databases. Titles and abstracts were screened followed by full-text review for inclusion criteria. Demographics and results were extracted from included articles.
Results
Ten studies met inclusion criteria and involved patients undergoing knee surgery and spinal surgery. IO lidocaine was shown to be effective for postoperative and intraprocedural pain control during vertebroplasty and kyphoplasty. IO morphine and IO NSAIDs were shown to be effective in reducing postoperative pain and opioid use after Total Knee Arthroplasty (TKA).
Conclusion
IO analgesia is a promising novel modality to improve pain control and decrease opioid usage in TKA, vertebroplasty, and kyphoplasty. Future research can evaluate whether IO analgesia is effective in additional orthopaedic procedures.
-

Invasive Pulmonary Aspergillosis: A Two-Year Journey
Jason Woods, Padmaditya Sureddi, Nga Van, and Danielle Ford
BACKGROUND: Highly active anti-retroviral therapy (HAART) has decreased the incidence of opportunistic infections among persons with HIV. Invasive aspergillosis specifically is uncommon among individuals with clusters of differentiation 4 (CD4) count >100 cells/mm3. Furthermore, treatment of aspergillosis in the HIV-infected population has not been examined systematically. We report a patient with CD4 count >200 cells/mm3, compliant with HAART therapy who developed invasive pulmonary aspergillosis (IPA) over the course of two years that was successfully treated through a combination of bronchial artery embolization and liposomal amphotericin.
CASE PRESENTATION: A 56-year-old man from southern Africa with four-year history of HIV-1 on HAART presented to the emergency department with complaint of hemoptysis that began the same day. He denied night-sweats, fatigue, or recent weight-loss, but reported that a suspicious area was discovered on chest imaging a year earlier. He also denied any history of smoking cigarettes, significant exposure to second-hand smoke, or respiratory irritants. On physical examination patient, his vital signs and lung exam were normal. His labs were remarkable only for a white blood cell count of 4.28K/µL. Computed tomography chest imaging demonstrated a mass-like consolidation along the medial aspect of the left upper lobe which appeared severely emphysematous, with moderate emphysema also present in other areas bilaterally. He was treated with a dose of tranexamic acid and empiric piperacillin/tazobactam.
He underwent a bronchoscopy, which identified a 5 cm lesion from which aspiration and biopsy samples were obtained. The pathology report revealed fungal forms suggestive of Aspergillus and blood fungitell assay was positive. He was treated with liposomal amphotericin B. He had persistent hemoptysis and subsequently underwent angiography which revealed abnormal vessels emanating from both the right and left bronchial arteries supplying the left upper lung and these were selectively embolized. Subsequent laboratory results were positive for urine strep antigen, but negative for detectable HIV-1 load, QuantiFERON-gold tested tuberculosis, Coccidioides antibody, urine Histoplasma antigen, and serum Aspergillus galactomannan antigen.
CONCLUSION: U.S. guidelines for management of IPA recommend starting patients on voriconazole. We present a case of IPA with HIV-associated emphysema in a patient from outside the U.S. treated initially with liposomal amphotericin B to mitigate concern for azole resistance and treated later with guideline-directed voriconazole after consulting resistance patterns.
LESSONS LEARNED: Management of nonnative patients with fungal infections should account for resistance patterns internationally. However, true prevalence of resistance in the US is unknown since routine antifungal susceptibility testing is not recommended.
-

Massive Subcutaneous Emphysema Following Robot-Assisted Total Laparoscopic Hysterectomy: A Case Report
Alia Valdez, Isabella Sciacca, and Charmaine Oladell
Background Subcutaneous emphysema is the presence of air within subcutaneous tissues, often presenting as swelling and palpable crepitus. Air may spread along fascial planes and arise from traumatic, iatrogenic, infectious, or spontaneous sources. In laparoscopic surgery, it is most commonly related to carbon dioxide insufflation. Reported incidence following laparoscopic procedures ranges from 2% to 24%, depending on procedure type, surgical duration, insufflation pressure, and patient factors. In gynecologic laparoscopy, incidence has been reported as low as 2.3% in some studies, with rates up to 10–15% in others, particularly with higher intraabdominal pressures. Although often benign, extensive subcutaneous emphysema may lead to significant complications, including airway compromise.
Case Report A 51-year-old woman with symptomatic uterine fibroids presented with chronic pelvic pain and heavy uterine bleeding and elected definitive surgical management. She underwent a planned robot-assisted total laparoscopic hysterectomy with bilateral salpingo-oophorectomy, lysis of adhesions, and cystoscopy. The patient was prepped and draped in the usual sterile fashion. During induction of anesthesia, difficulty with endotracheal intubation was noted; however, the airway was successfully secured, and the procedure proceeded as planned. The surgery was completed without apparent intraoperative complications. During the procedure, one trocar was inadvertently dislodged by the robotic arm and promptly reinserted. At the conclusion of the case, prior to extubation, extensive subcutaneous emphysema involving the abdomen, chest wall, neck, and face was noted upon removal of the surgical drapes. Vital signs remained stable, though the anesthesia team reported increasing ventilatory flow requirements during the procedure. Given concern for potential airway compromise from external compression, the decision was made to maintain endotracheal intubation. The patient was transferred to the intensive care unit for close monitoring and further management.
Lessons Learned This case highlights that while robot-assisted hysterectomy is generally safe, extensive subcutaneous emphysema remains a rare but clinically significant complication. Early recognition is critical, as extension to the neck and face increases the risk of airway compromise. Trocar dislodgement may contribute to extraperitoneal insufflation and should prompt reassessment of port integrity and insufflation parameters. Close collaboration between surgical and anesthesia teams is essential to guide airway management and postoperative disposition.
Conclusions Extensive subcutaneous emphysema following robot-assisted laparoscopic hysterectomy is uncommon but may have significant airway implications. Vigilance for atypical postoperative findings, careful management of trocar integrity, and prompt escalation of care are essential to ensuring patient safety and favorable outcomes.
-

Meconium Pseudocyst of the Perineum: Diagnostic Uncertainty and Surgical Management
Matthew Li, Muhammad T. Siddique, Charles Black, and James Davis
-

Navigating Recurrent Hematuria in Vesicular Varices: A Case of Successful Multidisciplinary Intervention
Morgan Grosdidier, Muiz Khan Tareen, and Danielle Ford
Background Hematuria secondary to vesicular varices is a rare but serious complication of portal hypertension, often associated with liver cirrhosis. Effective management requires a multidisciplinary approach, often involving urology, gastroenterology, and interventional radiology to address acute bleeding and prevent recurrence.
Case Presentation We present a case of a patient with alcoholic liver cirrhosis who experienced severe hematuria, highlighting the diagnostic and therapeutic challenges encountered. The patient presented with a two-day history of acute hematuria and blood clots, ultimately attributed to vesicular varices secondary to portal hypertension from alcoholic liver cirrhosis. Urology was consulted, who recommended continuous bladder irrigation (CBI), initially resolving the hematuria. Removal of the Foley catheter for a voiding trial resulted in recurrent hematuria that led to severe hypotension and a hemoglobin drop from 12 to 8 g/dL, necessitating rapid response and transfer to the intensive care unit. The patient received multiple blood transfusions and CBI was resumed. Gastroenterology was consulted to evaluate the need for esophagogastroduodenoscopy and assist with managing cirrhosis. In addition, interventional radiology was urgently consulted to also provide input for interventions. The patient underwent cystoscopy with fulguration of the bleeding varices, the largest of which measured approximately 2cm across. Due to the size of the varices and the high risk of rebleeding, the patient then underwent paraumbilical vein embolization to prevent further bleeding. There was no recurrence of hematuria afterwards and the patient was able to be discharged home in stable condition.
Lessons Learned/Conclusion This case underscores the importance of coordinated multidisciplinary care in managing complex hematuria due to vesicular varices in the context of portal hypertension. If not recognized early and properly managed, patients can suffer adverse effects such as exsanguination from rapid blood loss.
-

Negative Imaging, Ongoing Hemorrhage: An Ulcerated Jejunal AVM Requiring Advanced Endoscopic Intervention
Joel Mathews, Trina Lewis, John Mathew, and Long Hoang
Small bowel bleeding is relatively uncommon, accounting for less than 10% of all gastrointestinal (GI) bleeds. Small bowel angiodysplasias are the most common cause of small bowel bleeding. These lesions can often be difficult to identify on radiographic imaging or endoscopy and tend to rebleed after intervention. Our case centers on an 86-year-old patient who presented with an acute GI bleed from an obscure ulcerated jejunal arteriovenous malformation (AVM); his past medical history includes an undisclosed prior upper GI bleed treated with endoscopic clipping, paroxysmal atrial fibrillation, type 2 diabetes, prostate cancer with prostatectomy, and other chronic conditions. He presented for evaluation with symptomatic anemia from melenic stools. On admission, hemoglobin and hematocrit were 6.7g/dL and 22.9%, requiring 2 units of packed red blood cells to be transfused. Patient continued to have melena with persistent drops in hemoglobin throughout this admission requiring a total of 25 units of packed red blood cells along with IV iron infusions. The patient underwent small bowel enteroscopy (SBE) and Colonoscopy. SBE was grossly unremarkable. Colonoscopy revealed old blood but no active source of bleeding. Video capsule endoscopy (VCE) was performed which revealed trace amounts of old blood in the proximal small bowel with no clear etiology. A Tagged red blood cell scintigraphy was performed and determined that the source of bleeding was in the jejunum. A provocative CT angiogram was performed to localize and embolize the source however it was unsuccessful as there was no active extravasation noted during the study. Due to failed radiographic approaches to manage the patient’s ongoing bleed a repeat SBE beyond the extent of previous endoscopic reach was performed. The repeat SBE was notable for multiple jejunal arteriovenous malformations (AVMs), one of which was large and ulcerated and likely the etiology of notable blood loss requiring multiple blood transfusions. Argon plasma coagulation (APC) was performed on the smaller AVMs with successful ablation. APC along with endoclipping was performed on the ulcerated AVM resulting in successful ablation. The patient demonstrated rapid clinical improvement with resolution of melena, confirmed with a normalized hemoglobin, and he was eventually discharged. This case highlights the unique difficulty in diagnosing and managing an obscure type of small bowel bleed from ulcerated angiodysplastic lesions, as these produce greater blood loss but remain difficult to identify on mesenteric imaging and different types of endoscopy.
-

Nitrous Oxide vs. Ketamine: Impacts on Pediatric Emergency Department Length of Stay
Tabitha Brock and Anna Suessman
Background Nitrous oxide (N₂O) is a well-established analgesic and anxiolytic agent, widely used for procedural sedation in pediatric dentistry. Despite its demonstrated safety and efficacy, its use in Pediatric Emergency Departments (PEDs) remains limited and underexplored. To address this gap, we implemented a comprehensive training program for PED providers and introduced N₂O as an alternative sedation agent.
Objective We hypothesized that using N₂O for procedural sedation would significantly reduce patient length of stay (LOS) without compromising safety or outcomes.
Methods We conducted a retrospective chart review of pediatric patients who underwent painful procedures in a tertiary children’s hospital emergency department. The study was reviewed and approved by the hospital’s Institutional Review Board (IRB). The primary outcome was LOS in patients receiving ketamine versus N₂O. Secondary outcomes included procedure type and complications. Data for ketamine were collected from January 1, 2023, to December 31, 2024, and for N₂O from March 1, 2025 (its inception) to August 31, 2025. De-identified data were analyzed to compare LOS between the two sedation modalities using inferential statistics (independent samples t-test); side effects were descriptively summarized.
Results Out of 288 patients who received ketamine sedation, 260 met inclusion criteria, with a mean LOS of 459.40 minutes (Sd, 166). In comparison, 47 patients who received nitrous oxide (N₂O), 43 of whom met inclusion criteria, with a mean LOS of 190.95 (sd, 81.43) minutes. With a mean difference of 268 minutes (Welch’s t (111.1)=16.6, p < .001) and a large effect size (Cohen’s d = 1.71), this finding reflects a clinically and operationally meaningful reduction in LOS with N₂O. The most common procedures under ketamine were fracture reductions, followed by laceration repairs and abscess drainages. Under N₂O, laceration repairs were most frequent, followed by fracture reductions and abscess drainages. Hypoxia and nausea/vomiting occurred in 34% of ketamine cases, with hives reported in one patient. 3 In contrast, nausea, vomiting, or excitability occurred in 18% of N₂O cases.
Conclusion Nitrous oxide is a safe and effective procedural sedation option that significantly reduced LOS and is associated with fewer adverse events compared to ketamine. Implementing nitrous oxide as an alternative to ketamine enhances pediatric procedural care by significantly shortening LOS by over 4 hours, potentially reducing emergency department crowding and resource utilization while improving the patient experience.
-

Operative Localization of Occult Gastrointestinal Bleeding Using Intraoperative Small Bowel Endoscopy
Shuda Xia, Furrukh Jabbar, and Muhammad T. Siddique
-

Outcomes After ORIF of Closed Bimalleolar and Trimalleolar Ankle Fractures in Patients with Autoimmune Disease
McKenna Box, Troy B. Puga, Lachlan Anderson, Alyssa Kozlowski, and John T. Riehl
Background: Autoimmune disease is associated with chronic systemic inflammation, immunosuppressive therapy, and increased medical comorbidity, which may influence postoperative outcomes following fracture fixation. Data evaluating outcomes after ankle fracture surgery in this population remain limited. We hypothesized that autoimmune disease would be associated with higher postoperative complication rates following open reduction and internal fixation (ORIF) of closed ankle fractures.
Methods: We performed a retrospective cohort study using a multi-hospital dataset (2017-2025) to identify adult patients undergoing ORIF for closed bimalleolar or trimalleolar ankle fractures. Patients with autoimmune disease were propensity score matched 1:2 to patients without autoimmune disease based on age, sex, body mass index, Elixhauser Comorbidity Index, fracture pattern, and relevant medical comorbidities. Outcomes included acute care encounters (defined as presentation to the emergency department or hospital admission), thromboembolic events, postoperative medical complications, and fracture-related complications (malunion, nonunion, revision surgery), within 1 year. Rare outcomes were evaluated using Firth logistic regression.
Results: The matched cohort included 1,879 patients (autoimmune disease, n=627; controls, n=1,252), with well-balanced baseline characteristics. One-year acute care encounter rates were similar between groups (59% vs 58%, P=.72). Pulmonary embolism occurred more frequently among patients with autoimmune disease (5.4% vs 2.9%, P=.006), while rates of deep vein thrombosis were low and comparable. Rates of postoperative medical complications, including pneumonia, myocardial infarction, stroke, acute kidney injury, sepsis, and surgical site infection, did not differ between groups. Fracture-related complications were uncommon overall. Revision surgery or hardware removal within 1 year occurred less frequently in patients with autoimmune disease (0.3% vs 1.5%, P=.070). In adjusted analyses, autoimmune disease was not associated with mortality, acute care encounters, or postoperative medical complications but was associated with lower odds of fracture-related complications (OR 0.57, 95% CI 0.33–0.96; P=.033).
Conclusion: Autoimmune disease was not associated with increased acute care encounters, or overall postoperative medical complication rates following ankle fracture ORIF. Although pulmonary embolism occurred more frequently, fracture-related complications were less common. Autoimmune disease alone should not preclude standard operative management of ankle fractures, though thromboembolic risk may warrant closer perioperative attention.
-
 in Patients on Glucagon-Like-Peptide-1 Receptor Agonists (GLP-1a): A Systematic Review and Meta-analysis by Lachlan Anderson, Troy B. Puga, Erica Olfson, Kyle P. O'Connor, McKenna W. Box, and John T. Riehl")
Outcomes of Total Knee Arthroplasty (TKA) in Patients on Glucagon-Like-Peptide-1 Receptor Agonists (GLP-1a): A Systematic Review and Meta-analysis
Lachlan Anderson, Troy B. Puga, Erica Olfson, Kyle P. O'Connor, McKenna W. Box, and John T. Riehl
Introduction Glucagon-Like-Peptide-1 Receptor Agonist (GLP-1a) medications are commonly prescribed to treat diabetes and obesity, however, their effects on the outcomes of Total Knee Arthroplasty (TKA) remain largely unclear. The objective of this systematic review and meta-analysis is to evaluate the outcomes of patients undergoing TKA while using a GLP-1a medication.
Methods A search was conducted across MEDLINE/Pubmed, Cochrane, Google Scholar, Web of Science, and Embase databases. The search used a combination of keywords and Medical Subject Heading (MeSH) terms. Titles and abstracts were screened for eligibility. Full texts were then screened and included if they met eligibility criteria. Demographics and results were extracted from the articles that met inclusion criteria. Meta-analysis was conducted to evaluate outcomes.
Results Twelve studies, including over one million TKA patients, met inclusion criteria; eleven were retrospective and one was a prospective study. All included studies were of moderate quality. Six studies were applied to our meta-analysis, which showed GLP-1a use significantly reduced postoperative infection risk (OR 0.77, 95% CI 0.62–0.96; p=0.02) without increasing readmission, periprosthetic fracture, or overall complication rates. Limited long-term data showed GLP-1a use resulted in no detriment and possible benefits in revision reduction and discharge disposition.
Conclusion GLP-1a appear to be a safe adjunct for patients undergoing TKA, with consistent evidence of reduced infection risk and no increase in revision or overall complication rates. While certain subgroups may be more susceptible to short-term adverse events, the overall risk-benefit profile favors their use, particularly in obese and diabetic patients who face the highest perioperative risks. These findings support the growing role of GLP-1a medications in surgical optimization and highlight the need for prospective evaluation to guide standardized perioperative protocols.
-

Percutaneous Pneumothorax Placement
Miranda Bingham and Christopher Houston
Background: Timely and accurate chest tube placement in the Emergency Department (ED) is critical for the management of life-threatening conditions such as a pneumothorax. At Medical City North Hills Emergency Department, chest tube placement can be delayed or complicated due to variability in available equipment types, sizes, storage locations, and setup processes. Providers may be unfamiliar with less commonly used kits, experience skill decay due to infrequent procedural exposure, or lack access to bedside educational resources during high-stress, time-sensitive situations. These challenges contribute to procedural delays, increased complication rates, prolonged hospital stays, and higher healthcare costs. This quality improvement project aims to address these issues through the development and implementation of standardized, easily accessible instructional videos to improve procedural efficiency, provider confidence, and patient safety.
Methods: This initiative was conducted at Medical City North Hills Emergency Department and included emergency physicians, residents, advanced practice providers, nurses, respiratory therapists, and supply chain staff involved in chest tube placement. Short, standardized “how-to” videos were developed demonstrating appropriate chest tube and pigtail catheter selection, equipment setup, and insertion technique. Videos were made accessible via QR codes placed near chest tube kits and workstations, allowing providers to review content immediately prior to procedures. System-focused interventions included workflow modifications to support consistent kit retrieval and setup, while clinician-focused interventions targeted procedural education and refresher training. Complication rates associated with ED chest tube placements were tracked through manual chart review in Meditech during patient admission. Video utilization and provider feedback to be monitored to support iterative improvement.
Results: Implementation of standardized instructional videos improved provider familiarity with available equipment and reduced uncertainty during setup and insertion. Providers reported increased confidence in chest tube selection and placement, contributing to more efficient procedural workflows. Early tracking demonstrated a reduction in procedural delays and chest tube–related complications, including malposition, dislodgement, and the need for repeat attempts. Improved standardization also enhanced team communication and reduced time spent searching for supplies, supporting more reliable and consistent patient care.
Conclusion: The introduction of concise, standardized, QR code–accessible instructional videos effectively addressed key root causes of delayed and complicated chest tube placement in the ED. By improving provider confidence, streamlining equipment setup, and promoting consistent technique, this initiative enhanced patient safety, reduced complications, and supported high-quality emergency care.
-
 after a Distal Femur Non-Union: A Case Report by Troy Puga, Jenna Chrabolowski, McKenna W. Box, and Kisan Parikh")
Pigmented Villonodular Synovitis (PVNS) after a Distal Femur Non-Union: A Case Report
Troy Puga, Jenna Chrabolowski, McKenna W. Box, and Kisan Parikh
Background Pigmented villonodular synovitis (PVNS) is a rare benign neoplastic process that involves extensive proliferation of the synovium of a joint. Development of PVNS has been potentially linked to traumatic etiologies, however, evidence for this remains limited. This case report aims to present a case of PVNS that developed after a traumatic etiology.
Case Presentation A 62 year old female presented with recurrent left knee effusion and non-union of the left distal femur roughly four years after an MVC and index open reduction and internal fixation with a lateral locking plate and screw construct. Left knee aspiration at initial visit revealed hemorrhagic fluid. Advanced imaging, laboratory workup, and bone biopsy were obtained to rule out potential causes of the non-union. All workup provided no underlying etiology for the non-union or knee hemarthrosis. The patient underwent non-union revision with hardware removal, intramedullary nailing and bone graft placement. Due to concern for the recurrent knee effusion, the knee joint was evaluated which revealed synovitis and hemosiderin deposits. The patient underwent extensive synovectomy, and pathological specimens confirmed results consistent with PVNS. The patient returned for follow-up, and no-longer was developing knee effusions at most recent follow-up (12 weeks from index procdure).
Lessons Learned PVNS can occur after a traumatic injury, and diagnosis remains challenging.
Conclusion PVNS can occur after a traumatic injury, and this case report highlights the first case of PVNS of the knee after a distal femur fracture with subsequent non-union. Surgeons should consider PVNS for recurrent joint effusion after traumatic injuries.
-

Prognostic Impact of Sentinel Lymph Node Dissection in High-Risk Uterine Serous Carcinoma
Katie Johnson, Chrystal Stallworth, Prakriti Srivastava, Abel Moron, Brandon Roane, Hannah Affleck, and Michele McCarroll
Objective: To assess overall survival (OS) for patients undergoing surgical staging with sentinel lymph node dissection (SLND) in patients with high risk uterine serous carcinoma (USC).
Methods: Patients diagnosed with USC that underwent surgical staging with SLND from the years 2018-2022 were included for analysis utilizing the Surveillance, Epidemiology, and End Results (SEER) national database. Patients were stratified by pathologic lymph node (LN) assessment into true SLND group (1-2 pelvic LN retrieved) and false SLND group (> 2 pelvic LN retrived). Patients with 0 LN retrieved were excluded from the data. OS was recorded in months from time of primary treatment to death or loss to follow up. Chi-square analysis and ANOVA was used to evaluate the data set for impact of lymph node count OS between the two categorical groups; true and false SLND.
Results: A total of 524 patients met inclusion criteria. Patients ranged from ages 35-85+ with a median age range of 70-74. Racial/ethnic distribution included 55.3% Non-Hispanic White, 21% Non-Hispanic Black, 11.5% Hispanic, 11.6% Asian/Pacific Islander, and 0.6% American Indian/Alaska Native. Of the patients included in the study, 34.5% (n=175) met true SLND group stratification and 65.5% (n=343) were in the false SLND group. Staging descriptives are as follows; 69.6% stage 1, 5.3% stage 2, 18.7% stage 3, 5.8% stage 4, and 0.6% were unknown at time of diagnosis. Of these, 57.8% of patients underwent adjuvant radation (RT) with no patients in either group receiving neoadjuvant RT. Negative peritoneal washings were found in 56.9% of patients, positive washings in 11.1% , and suspicious or atypical washings in 5.0%. A total of 143 pts (27.2%) had additional sampling of the para-aortic lymph nodes (PALN), with greater PALN assessment in the false SLND group (p< 0.001). Unadjusted mean OS was 18.54 mos. in the true SLND group vs 19.59 mos. in the false SLND cohort (p=0.3639). Approximately 34.2% patients had survival ≥ 25 mos. As expected, adjuvant chemotherapy (p = 0.003) conferred increased OS. Conversely, higher grade (p = 0.006), and advanced stage (p =0.021) were all statistically associated with decreased OS. No other significant differences were found for age (p=0.563), race, peritoneal washings status (p=0.51), or radiation sequence; defined as either radiation after surgery versus no radiation or unknown radiation.
Conclusion: SLND has become a widely adopted staging technique in recent years, and has repeatedly shown good diagnostic value for both low and high risk populations. However, its prognostic significance and impact on long-term OS in high risk patients including USC warrants continued investigation. This study highlights the variability of pathologic lymph node count return in patients undergoing presumed SLND. Additionally, we found no statistical association between higher pathologic LN assessment and OS. Our results further emphasize that SLND remains a valuable diagnostic and prognostic tool for patients with high risk USC.
-

Prognostic Value of Systemic Inflammatory Indices for Predicting MACE in NSTEMI Patients Undergoing PCI
Boney Lapsiwala, Aditya Sharma, Usman Khan, Jorim Parmar, Justin Soloman, Veeranna Vibhuti, and Mehdi Khalafi
Background: Cardiovascular diseases (CVD) account for nearly one-third of global mortality, with ischemic heart disease caused by a mismatch between myocardial oxygen supply and demand. Despite advances in percutaneous coronary intervention (PCI) and contemporary pharmacotherapy, patients with non–ST-segment elevation myocardial infarction (NSTEMI) continue to experience substantial residual risk for major adverse cardiovascular events (MACE). As traditional risk stratification tools have limited ability to identify high-risk individuals, interest has shifted toward biomarkers reflecting inflammatory pathways central to atherosclerosis and plaque instability. Hematologic inflammatory markers including pan inflammatory value (PIV), systemic immune inflammation index (SII), neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR) initially validated in oncology, have emerged as promising predictors of cardiovascular disease.
Methods: We performed a retrospective analysis of the North Texas healthcare database including adults (≥18 years) hospitalized for chest pain (2016–2024) with NSTEMI defined by ESC criteria who underwent successful PCI of culprit vessel. Patients were stratified into MACE and non-MACE cohorts, followed for 7 days from index hospitalization. MACE comprised heart failure (HF), ischemic stroke (IS), in-stent restenosis (ISR), malignant arrhythmia (MA), cardiac arrest (CA), in-hospital mortality (IHM) and cardiogenic shock (CS). ROC curve analysis was used to determine the performance of the PIV, SII, NLR and PLR.
Results: Among 1,945 patients with NSTEMI, 805 experienced MACE. Compared with the non-MACE cohort, patients with MACE were older (median age 69.5 vs 62.0 years), longer hospital length of stay (4 vs 2 days), and a higher prevalence of diabetes and hyperlipidemia. The MACE cohort included a slightly higher proportion of females and Hispanic patients, with lower proportions of males, White, and African American patients. Patients with MACE demonstrated higher neutrophil and platelet counts with lower lymphocyte counts, while monocyte levels were similar between groups. Inflammatory indices were consistently higher in the MACE cohort, including PIV (589.2 vs 429.6), SII (830.9 vs 643.8), PLR (135.8 vs 116.8), and NLR (3.8 vs 2.8). HF accounted for the majority of MACE events (89.01%), followed by MA (11.62%), CS (9.71%), IHS (6.69%), IS (4.78%), CA (4.62%), ISR (0.96%); cardiogenic shock in 42 patients. ROC analysis demonstrated modest discriminative performance for MACE, with AUCs of 0.588 for PIV, 0.584 for SII, 0.597 for NLR, and 0.570 for PLR.
Conclusion: Readily available hematologic inflammatory indices were higher among NSTEMI patients experiencing early MACE following PCI, underscoring the role of systemic inflammation in short-term post-NSTEMI risk and supporting the need for prospective validation.
-

Pulse Check: IM Resident Wellness Initiative -- A Continuous QI Project
Jacqueline Bekhit, Ngoc Vu, Yasasvi Sabbineni, Nihar Raju, Parth Patel, and Teena Mathew
Background Burnout is a psychological syndrome that arises from chronic workplace stress that has not been effectively managed. It is characterized by emotional exhaustion, increased mental distance or cynicism toward one’s work, and a sense of reduced professional efficacy (WHO, 2019). Due to the long work hours, high workload, and extensive training demands, medical residents are particularly vulnerable to experiencing burnout, contributing to higher rates of anxiety and depression. Burnout typically emerges mid-intern year and progresses through the remainder of residency. Burnout can contribute to higher medical errors, decreased work efficiency, and poor patient-physician interactions.
Methods This QI is a continuous project involving all residents in the HCA Medical City Healthcare Internal Medicine Program. Conducted in collaboration with the Wellness Committee, the initiative included recurring scheduled wellness events and educational lectures. Wellness lectures addressing burnout recognition, coping strategies, and substance use were incorporated into the curriculum. Resident wellness and burnout were assessed through online surveys administered twice yearly via Google Forms. The survey at the beginning of the year will include questions about expectations, and any events the resident would like to participate in. A survey at the end of the year will evaluate the residents’ wellness by using the Resident Wellness Score and to evaluate the events that occurred during the year. Survey data were reviewed iteratively by the QI team to inform ongoing refinement of wellness planning and support continuous improvement in resident wellness.
Results The results are assessed through surveys given twice a year that evaluate residents’ overall well-being and provide an opportunity for them to share feedback. Baseline survey data will be collected to establish resident wellness metrics and guide event planning for the following year. Ongoing data collection will evaluate longitudinal trends in wellness domains and perceived burnout. As this project is currently at the early stages, results are not available at this time.
Conclusion Implementation of structured wellness events and structured lectures can address key contributors to resident burnout. Establishing consistent assessment and targeted interventions may improve resident well-being, foster community, and support sustainable training environments."
-

QI Project: Improving Utilization of Cardiac Monitoring on Inpatients Based on AHA Guidelines
Muhammad Humais, Jorim Parmar, Shakir Al-Ezzi, Florence Murray, David Maldonado, and Mohan Sengodan
-

Reconsidering Routine Postpartum Complete Blood Count in Uncomplicated Vaginal Deliveries: A Quality Improvement Project
Mira Ibrahim, Katie Johnson, Isabella Sciacca, Ali Ohm, and Nicole Tenzel
BACKGROUND
While a postpartum CBC may be helpful to detect anemia, it may not be necessary in a routine, uncomplicated patient and may be more of a burden and cause inconvenience without providing significant benefit. The goal of our project is to have a positive impact on patient care, hospital efficiency, and healthcare cost for both hospital and patient.
METHODS
Using data from July 2025 onwards for a six-month period is the intended duration of our study. We are looking at which patients got a postpartum CBC (which is usually collected one day after delivery) and whether that lab draw was necessary in that it resulted in a change in the patient’s postpartum management. Criteria for obtaining a CBC in our study are as follows: cesarean or operative vaginal deliveries, spontaneous vaginal delivery with PPH (QBL >1000cc), admission hemoglobin of < 10, anemia symptomatology, hemodynamic instability, risk factors for postpartum hemorrhage (chorioamnionitis, multiparity, history of PPH), known bleeding disorder, or CBC ordered for other reasons (preeclampsia). Only vaginal deliveries for patients who are a part of the graduate medical education (GME) or drop-in patients (those admitted to Medical City Arlington but who were receiving care by an outside physician) were included.
RESULTS
Current data for our study includes 99 deliveries, 38 of which were vaginal deliveries. 32 of these deliveries got a postpartum CBC, 10 of which were not warranted based on the criteria outlined above. All 10 of these CBCs did not lead to a change in management in the postpartum period. Additionally, 6 of the 38 vaginal deliveries did not get a CBC when one was not warranted, and this also did not make a change in their postpartum management.
CONCLUSION
With additional cycles of our study, we will obtain more data to underscore our conclusion and validate our original hypothesis. Thus far, the results of our study demonstrate that for relatively uncomplicated vaginal deliveries, a postpartum CBC is not warranted and does not result in a change in management of the patient. If a lab test (in this case a CBC) is not drawn because it is not warranted, this is not only beneficial to a patient because it avoids an unnecessary blood draw, but it also reduces cost to the hospital and burden on lab technicians and is an easy and worthwhile step to implement at any healthcare facility.
-

Reducing Respiratory Viral Testing in a Pediatric Emergency Department: A Quality Improvement Initiative
Anna Suessman
Background: Respiratory viral testing in pediatric emergency departments (EDs) is frequently performed despite limited impact on clinical management for many low-risk presentations. Unnecessary testing increases cost and operational burden may delay patient throughput and can provide false reassurance to caregivers. Additionally, pediatric emergency department nurses agreed with overburden and impact to throughput based on overuse of viral testing (qualitative nursing survey conducted on September 4, 2024 showed >98% felt testing was unnecessary). We hypothesized that reducing testing through standardized team education and discharge processes would not negatively affect patient experience. This initiative aimed to decrease unnecessary respiratory viral testing during respiratory season by implementing a standardized “Swab & Go” workflow supported by clinician and nursing education and standardized discharge instructions.
Methods: We conducted a pre/post quality improvement evaluation in a pediatric ED. Baseline respiratory viral test orders by provider were collected from September 2023 through February 2024. A staged intervention PDSA bundle was implemented, including clinician group discussion (June 17, 2024), Swab & Go pathway revision (July 1, 2024 to the previously published pathway from February 1, 2024), education on appropriate indicators for testing (July 23, 2024) and standardized discharge instructions for families (August 30, 2024). Post-intervention monthly data were collected from September 2024 through February 2025 and compared with the baseline season. The primary outcome was respiratory viral tests per ED visit (tests/visit). Provider-level performance was measured against a goal of ≥50% reduction from baseline. The “Swab & Go” pathway applied to children older than 12 months who were discharged home with reassuring vital signs and a presumed viral respiratory illness.
Results: During the baseline period (September 2023–February 2024), testing averaged 1.19 tests per visit across 20,810 visits. In the post-intervention period, testing decreased to 0.47 tests per visit across 10,283 visits, representing an absolute reduction of 0.72 tests per visit (72 fewer tests per 100 visits) and a 60.5% relative reduction. Fifteen of sixteen providers reduced respiratory viral testing overall with 10/17 providers decreasing by 60% in this short timeframe since intervention.
Conclusions: Implementation of a standardized “Swab & Go” pathway with staged multidisciplinary education and discharge standardization significantly reduced respiratory viral testing in a pediatric ED. Importantly, patient experience scores improved during the intervention period and remained above the national 75% top-box benchmark.
-

Relationship Between Exception Request for Higher Listing Urgency and Aggressiveness in Accepting Heart Offers
Jorim Parmar, Yingxian Liu, Devika Adusumilli, Luke Taylor, Shakir Al-Ezzi, Usman Khan, Claudio Bravo, Claudius Mahr, and Song Li
BACKGROUND: Transplant programs may submit exception requests to upgrade a listed patient’s priority, often anticipating a higher likelihood of accepting marginal or high-risk donor organs. This study explores whether exception request status is associated with increased risk tolerance in organ acceptance.
METHODS: We conducted a retrospective analysis using data from the Scientific Registry of Transplant Recipients (SRTR), focusing on adult patients (≥18 years) listed for heart transplantation. Statistical analyses were performed using SAS/STAT 14.1. Descriptive statistics summarized demographic and clinical variables. Baseline characteristics were compared between recipients with and without exception requests. Primary analysis: Mixed-effects linear regression was used to model continuous risk scores, incorporating a random intercept for transplant center and adjusting for recipient factors including age, sex, mechanical support devices, comorbidities, left ventricular hypertrophy, cardiac output, race, and HCV status. Secondary analysis: Logistic regression assessed the likelihood of accepting high-risk donor organs, defined by thresholds at the 75th, 80th, and 90th percentiles.
RESULTS: Among 20,543 heart transplant recipients, the average candidate age was 53.3 years (±12.8), with 72.9% male and 27.1% female. Racial distribution included 68.5% Caucasian, 25.6% Black, 4.0% Asian, 0.5% Multiracial, and 1.4% Other. Hispanic ethnicity accounted for 11.1% of candidates. Donor candidates had an average age of 33.0 years (±10.2) and an average ejection fraction of 61.8% (±6.8). The average recipient length of stay was 24.6 days (±27.4). Further analyses will explore stratified predictors of mortality, donor characteristics, and diagnostic indicators such as ejection fraction, wait time, and hospitalization duration.
CONCLUSION: This study aims to determine whether exception requests are associated with increased risk tolerance in organ acceptance, potentially informing transplant center practices and allocation policies.
-

Rethinking Acute Pain Management: Evidence for Suzetrigine as an Opioid-Sparing Strategy in Outpatient Care
Shana-Kay Lambert-Johnson and Tasaduq Mir
BACKGROUND: The ongoing opioid epidemic underscores the urgent need for effective nonopioid options for acute pain management. Suzetrigine, a selective voltage-gated sodium channel NaV1.8 inhibitor, represents a mechanistically novel analgesic targeting peripheral nociception and may reduce reliance on opioid therapy. It received FDA approval on January 30, 2025, for the treatment of moderate-to-severe acute pain in adults. This evidence-based review evaluates the efficacy and safety of suzetrigine as an opioid-sparing option for outpatient acute pain management.
METHODS: A structured literature search of PubMed was conducted from database inception through January 2026 using the terms “suzetrigine” and “NaV1.8.” Eligible studies were randomized, double-blind, controlled trials enrolling adults (≥18 years) with moderate-to-severe acute pain (numeric pain rating scale ≥4) treated with suzetrigine and reporting validated pain outcomes. Phase 1 pharmacokinetic studies without efficacy endpoints were excluded.
RESULTS: One randomized controlled trial publication met inclusion criteria, reporting outcomes from two phase 3 trials involving patients undergoing abdominoplasty (n=1,118) and bunionectomy (n=1,073). In both trials, suzetrigine administered as a 100-mg loading dose followed by 50 mg every 12 hours produced statistically and clinically significant reductions in pain intensity compared with placebo over 48 hours, measured by the time-weighted sum of pain intensity difference (SPID48). Adjusted mean treatment effects favored suzetrigine by 48.4 points in the abdominoplasty trial (95% CI 33.6–63.1; P< 0.0001) and 29.3 points in the bunionectomy trial (95% CI 14.0–44.6; P=0.0002). Analgesic efficacy was comparable to hydrocodone bitartrate/acetaminophen (5/325 mg every 6 hours), with neither study demonstrating superiority over the opioid comparator for the primary outcome. Suzetrigine demonstrated a faster onset of clinically meaningful pain relief than placebo. Rates of nausea and vomiting were lower with suzetrigine than with opioid therapy, and treatment discontinuation due to adverse events was uncommon (0.6%). No evidence of respiratory depression, sedation, abuse potential, or withdrawal symptoms was observed.
CONCLUSION: Current evidence suggests that suzetrigine provides effective analgesia comparable to opioid therapy for acute postoperative pain, with a more favorable safety and tolerability profile. These findings support its potential role as an opioid-sparing option in outpatient acute pain management. However, available evidence is limited to short-term postoperative settings in relatively healthy adults. Further studies are needed to evaluate its effectiveness in nonsurgical acute pain conditions, broader patient populations, and real-world opioid-sparing outcomes.
-

Retrospective Analysis of Predictive Accuracy in Applying the NIH Stroke Scale
Rachel Hoang, Ray Rahimi, Kelly Mofor, Charley Meadows, Ty Shields, Hibba Thayyil, Hannah A. Affleck, Parker Owen, and Sanjay Sharma
BACKGROUND: The National Institutes of Health Stroke Scale (NIHSS) is widely used to quantify neurologic deficits in acute stroke, yet it is based on observable symptoms rather than ischemic stroke pathophysiology. Because ischemic stroke typically results from focal vascular occlusion, deficits classically localize to a single hemisphere and do not cross the midline. The frequency with which patients presenting with bilateral or contralateral symptoms have MRI-confirmed ischemic infarction, compared with those with unilateral deficits, remains unclear.
METHODS: We performed a retrospective analysis of patients for whom a code stroke was activated at a single institution. Patients presenting with bilateral/contralateral or ipsilateral neurologic deficits were included. Initial NIHSS scores were recorded, and MRI reports were reviewed for evidence of ischemic infarction. Patients receiving tenecteplase or lacking documented NIHSS or MRI were excluded. Associations between NIHSS score, symptom laterality, and imaging-confirmed stroke were examined.
RESULTS: A total of 268 patients met inclusion criteria. The cohort ranged in age from 34 to 85+ years. Of the patient population, 46.6% were male and 53.4% were female. History of a cardiac event was 97%, with 22% of the population identifying as smokers. Patients with contralateral or bilateral deficits were 9.3%, while 43.3% of the population had ipsilateral. Patients were assigned a NIH Stroke Scale Score, with 23.1% with No Stoke (0), 42.9% with Minor Stroke (1-4), 27.6% with Moderate Stroke (5-15), 3% with Moderate to Severe Stroke (16-20), and 3.4% with Severe Stroke (21-42). Ischemic stroke was evaluated on MRI, with 75% positive and 25% negative. The proportion of patients with positive MRI findings did not differ significantly between those with bilateral or contralateral deficits and those with unilateral deficits (72% vs 75%; p>0.7)
CONCLUSION: Although contralateral neurologic findings were less common, most patients with these presentations had MRI-confirmed ischemic stroke. While ischemic stroke typically produces unilateral deficits, contralateral symptoms do not exclude focal infarction. Reliance on symptom laterality or symptom-weighted scales such as the NIHSS may incompletely reflect stroke pathophysiology and should be interpreted alongside neuroimaging. Emergency clinicians should maintain a high index of suspicion and prioritize imaging when stroke is suspected, regardless of deficit laterality.
-

Robotic Cholecystectomy with Choledochoscopy After Failed ERCP: A Case Report
James Zhang, Ethan Pavlovsky, Jennifer Austin, Furrukh Jabbar, and Hassan Ahmed
Background: In the United States, there are an estimated 20 million cases of cholelithiasis, though a majority remain asymptomatic. Development of choledocholithiasis is seen in 10%-20% of those with cholelithiasis. Typically, choledocholithiasis is managed via a two-stage approach starting with endoscopic retrograde cholangiopancreatography (ERCP) followed by laparoscopic cholecystectomy on the same admission. More recent trends have seen a shift towards surgeon-directed management of the common bile duct through one-stage procedures that combine cholecystectomy with intraoperative common bile duct (CBD) exploration using choledochoscopy. We present a case of chronic choledocholithiasis with large, impacted gallstones that was managed with robotic cholecystectomy, choledochotomy, and choledochoscopy after failed ERCP.
Case Presentation: An 86-year-old female presented with a 2-month history of abdominal pain with associated weight loss and decreased oral intake. The patient was initially seen at an outside hospital where CT imaging revealed cholecystitis and choledocholithiasis with two large 2-cm CBD stones. ERCP was attempted but duct cannulation was unsuccessful due to a duodenal stricture. The patient was transferred to our facility where the patient was taken to the operating room and a robotic choledochotomy was created with subsequent choledochoscopy. Two large impacted CBD stones were identified and successfully cleared from the duct with a combination of electrohydraulic lithotripsy, wire snare, irrigation, and manual manipulation. A robotic cholecystectomy was then performed. The patient was discharged from the hospital on postoperative day 3 without the need for any further intervention.
Discussion and Conclusion: Choledocholithiasis management currently has an evolving treatment landscape. The introduction of intraoperative choledochoscopy offers a modern, minimally invasive, single-stage method for CBD exploration and stone elimination, thereby reducing the dependence on gastroenterology (GI) intervention and avoiding added risks associated with ERCP. Furthermore, common bile duct exploration is the current bail out procedure after failed ERCP further supporting the expansion of minimally invasive choledochoscopy. This case suggests minimally invasive intraoperative choledochoscopy is a safe and effective treatment for managing complex choledocholithiasis, even in patients who have failed ERCP.
-
 and Vitamin D Levels in Asthma Severity and Length of Stay by Kumail Rizvi, Kenny Tran, Michele McCarrol, and Mohan Sengodan")
Roles of Thyroid Stimulating Hormone (TSH) and Vitamin D Levels in Asthma Severity and Length of Stay
Kumail Rizvi, Kenny Tran, Michele McCarrol, and Mohan Sengodan
Background: Asthma exacerbations leading to hospitalization are very common and result from multifactorial causes. This research aims to investigate factors such as thyroid-stimulating hormone (TSH) and Vitamin D, which may play a role in the modulation of asthma-related hospitalizations and patient outcomes. TSH influences numerous cellular processes in the body, particularly during times of stress and illness, yet its role in asthma exacerbations and hospital length of stay remains unclear. Vitamin D has been studied for its role in enhancing medication absorption and regulating immune function, and multiple studies have shown that low serum Vitamin D levels are associated with greater asthma severity, poor asthma control, and more frequent exacerbations. While Vitamin D is commonly evaluated in the context of hypocalcemia, it is not routinely measured during asthma exacerbations in hospitalized patients, despite its potential role in preventing future exacerbations by supporting critical cellular self-regulatory processes. From a preventive care perspective, this research seeks to determine whether maintaining normal levels of TSH and Vitamin D, compared to low or high levels, impacts hospital length of stay.
Methods: This study is designed as a retrospective study of patients diagnosed with asthma exacerbations requiring inpatient admission. Patient data were obtained from the HCA patient database at a divisional level. Inclusion criteria included patients 18 years and older who were admitted with at least one specific CPT or ICD code indicating an asthma exacerbation. Furthermore, TSH and/or Vitamin D levels must have been ordered during the patient’s hospital course. Both length of stay and 30-day readmission rates were analyzed.
Results/Conclusion: Patients meeting inclusion criteria have been identified via the HCA database, and statistical analysis is currently underway. The two current working hypotheses are as follows: (1) adults diagnosed with Vitamin D insufficiency or deficiency have a longer length of stay and/or more severe asthma exacerbations compared to those with normal Vitamin D levels, and (2) adults with controlled TSH levels have a shorter hospital length of stay for asthma exacerbations compared to those with uncontrolled TSH levels.
-

Salvage Percutaneous SpyGlass-Assisted Lithotripsy via a Cholecystostomy Tract After Failed ERCP: A Case Report
Nicholas Gerden, Tiffany Hong, Asad Rehman, and Long Hoang
IR-driven percutaneous cholangioscopy with SpyGlass-assisted lithotripsy is an emerging salvage technique for biliary stone disease in patients with failed or contraindicated endoscopic retrograde cholangiopancreatography (ERCP) due to complex anatomy. We report an 85-year-old patient with an indwelling cholecystostomy tube and biliary stent who presented with recurrent obstructive jaundice, with cholangiography demonstrating occlusion of the common bile duct stent due to choledocholithiasis. Conventional ERCP was unsuccessful because of complex biliary and gastrointestinal anatomy. A multidisciplinary interventional radiology–gastroenterology approach was therefore pursued, utilizing antegrade percutaneous choledochoscopy through an existing cholecystostomy tract with SpyGlass-assisted lithotripsy, followed by cholecystostomy tube exchange. The procedure resulted in successful ductal clearance, no major periprocedural complications, and complete resolution of symptoms. This case highlights the safety and feasibility of SpyGlass-assisted lithotripsy via a cholecystostomy access route as a minimally invasive salvage strategy and underscores the importance of multidisciplinary collaboration in the management of complex biliary stone disease.
-

Septic Arthritis Suspected but Pseudogout Confirmed: The Importance of Early Joint Aspiration and Crystal Analysis
Munazzah Kaleem and Jose Lozano
BACKGROUND/ INTRODUCTION: Septic arthritis present as an acute monoarticular arthritis and is highly suspected in patients with risk factors including DM, ESRD, and bacteremia. As a result, empiric antibiotics are usually started prior to definitive diagnosis. But crystal induced arthropathies closely mimic septic arthritis in their presentation. This case highlights the importance of early arthrocentesis to avoid unnecessary antibiotic treatment.
CASE PRESENTATION: 50-year-old female on antibiotics for MSSA bacteremia presented due to acute onset left hip pain, swelling and decreased range of motion. No trigger was present. PMH included HTN, T2DM and ESRD on HD. She denied fever, chills or any other systemic symptoms. Labs demonstrated WNL leukocytes. CT scan showed moderate size left femoral acetabular joint effusion with surrounding synovial hyperemia and bilateral iliopsoas hematoma. Based on recent history of MSSA working diagnosis was made as septic arthritis which prompted us to start her on antibiotics. arthrocentesis was performed and fluid was sent for studies after starting her on antibiotics. Fluid shows mild inflammation with no concern for septic arthritis. Suspicion was still high for septic arthritis given the recent diagnosis of MSSA, and it was thought that fluid studies were negative as patients have been on long term antibiotics. The case took an interesting turn when fluid studies showed bifringent crystals consistent with CPPD; Pseudogout and G/S and culture remained negative. The patient started and responded well to steroids.
DISCUSSION: This case shows how pseudogout mimics gout, especially in patients having risk factors for septic arthritis. Recent MSSA bacteremia and acute onset of hip symptoms justifiably raised concerns for septic arthritis prompting early antibiotic initiation. However, proper diagnostic tests lead to diagnosis. CPPD is underdiagnosed with a prevalence of 4-7% of the adult population in USA and Europe and is rarely seen in patients younger than 60 years. It is commonly presented as a painful and swollen joint which makes it difficult to distinguish from septic arthritis. Synovial fluid analysis and crystal studies are the mainstay for diagnosis and distinguishing it from septic arthritis.
TEACHING / LEARNING POINTS: Arthrocentesis and fluid studies should be done early, ideally before antibiotic initiation, in cases concerning arthritis and having effusion to r/o aseptic arthritis. As aseptic arthritis can get masked under septic arthritis.
-

Stronger Together: A Resident-Led Initiative Advancing School Nurse Readiness in Pediatric Seizures and Pediatric Cardiology
Shana-Kay Lambert-Johnson, Amy Nguyen-Pham, Tony Do, Devika Adusumilli, Jorim Parmar, Dimitar Semerdzhiev, Elizabeth White, Joanna John, Myrna Garcia, Nicholas Gerden, Tasaduq Mir, and Michele McCarroll
BACKGROUND: School nurses play a vital role in safeguarding the health and safety of children by serving as frontline providers within the school setting. Timely recognition and appropriate management of acute medical conditions can reduce morbidity, prevent unnecessary emergency department utilization, and improve long-term outcomes. Needs assessment surveys identified knowledge and confidence gaps among school nurses related to pediatric seizure management and pediatric cardiology.
METHODS: This prospective educational quality improvement initiative was conducted across the Dallas–Fort Worth (DFW) region during the 2025-2026 academic year. Over 25 residents served as curriculum developers and educators, creating and delivering evidence- and case-based education focused on seizures and pediatric cardiology across Medical City Healthcare facilities. A pre-intervention learning needs assessment survey identified and prioritized essential topics. The target audience included school health professionals from approximately 30 school districts. Educational modalities included online modules, in-person lectures, and simulation-based cases tailored to school settings, delivered across 26 sessions. Program evaluation followed Kirkpatrick’s four levels (Reaction, Learning, Behavior, Results) using post-session surveys incorporating Likert-style items, Net Promoter Score, and open-ended responses completed by participants receiving Continuing Nursing Education (CNE) credit.
RESULTS: Interim program evaluation demonstrated that 870 participants attended the sessions in 2025, with 11 remaining sessions scheduled in 2026. Attendees included Registered Nurses, Licensed Practical Nurses, Certified Nursing Assistants, Medical Assistants, Clinic Aides, and allied school health personnel. At the conclusion of the sessions, 89% (n=774) of participants reported they would implement changes in their clinical practice or apply the knowledge gained. 97% of respondents reported gaining new knowledge or reinforcement of existing knowledge. Nurses rated the presentations highly, with an average score of 4.8 out of 5, and the program achieved a Net Promoter Score of 80%, equating to a "World Class" designation. These findings demonstrate high engagement and meaningful educational impact among participating school health professionals.
CONCLUSION: This resident-led educational initiative improved school nurse knowledge, confidence, and preparedness in managing pediatric seizures and pediatric cardiology conditions across DFW public schools. The program highlights the dual impact of resident leadership in community education: enhancing school-based pediatric readiness while advancing resident ACGME core competencies in medical knowledge, systems-based practice, leadership, and interprofessional communication. This scalable model demonstrates how empowering residents as educators and leaders can simultaneously strengthen population health outcomes and graduate medical education.
-

Surgical Management of a Giant Colonic Diverticulum
Courtney Koplyay, Mason Workman, Michael Truitt, and Muhammad T. Siddique
INTRODUCTION: Giant colonic diverticulum (GCD), defined as a diverticulum >4 cm, is a rare manifestation of diverticular disease with less than 200 reported case reports. CT imaging is the preferred imaging modality to identify and confirm the presence of a GCD, which provides an accurate depiction of the size, location, and contents of the diverticulum GCD can present with nonspecific abdominal symptoms, abdominal pain, bloody stools, or an enlarging mass. Given the risk of serious complications, including diverticulitis, bowel obstruction, and perforation, early recognition and management are essential to prevent further complications. Surgical management with diverticulectomy or partial colectomy is the first-line management for definitive management of GCD.
CASE PRESENTATION: A 57-year-old male presented with an enlarging abdominal mass and was found to have a 10 cm giant colonic diverticulum in the sigmoid colon. The patient was successfully managed with an open partial colectomy and primary colonic anastomosis.
LEARNING POINTS: Giant colonic diverticula remain a rare but clinically significant presentation of diverticulosis. While laparoscopic or robotic technique is often preferred, there is a concern of increased risk of bowel perforation with instrument manipulation. Open partial colectomy is a reasonable alternative for patients with high risk of diverticular rupture to prevent intraoperative complications while offering definitive management of GCD.
-

Survival Outcomes Following Thyroidectomy in Secondary Thyroidal Metastases
Hannan Maqsood, Tanya Odisho, Yaqeen Qudah, Umar Butt, and Awni Shahait
Background: The management plan for metastasis to the thyroid from distant primary malignancies remains unclear. Methods: This systematic review is being conducted to evaluate the outcomes for performing thyroidectomy in non thyroidal metastatic cancer. Data: Data was collected via literature search using pubmed, cochrane, web of science, and google scholar.
PICO:
- Population: Patients undergoing thyroidectomy in nonthyroidal metastatic from distal primary cancer
- Intervention: Thyroidectomy (lobar/total)
- Comparison: No comparison group
- Outcomes: Overall survival Locoregional Recurrence Mortality
Results: As per literature review, renal cell carcinoma was most common, (around 30-35%) patients, followed by lung and gastrointestinal malignancies. Surgical management was associated with improved survival duration (P < .01). Locoregional recurrence was less likely in patients treated with total versus partial thyroidectomy (4.8% vs 13%). Extent of surgical management did not have a significant effect on patient survival. The median survival from surgery to death or last follow-up was ranged 2-114 months. In the literature review cohort, the OS of patients with RCC thyroid metastasis was 213.6 months, and there was no statistically significant survival difference based on the site of metastasis. Median survival after thyroid metastasis from RCC for the literature cohort was 45.6 months, respectively.
Conclusion: Surgical intervention is associated with improved survival, but expected morbidity of untreated tumors is difficult to assess. Site of origin, time to diagnosis, and surgical approach are related to survival and recurrence rates.
-

Tales from the Cryptogenic: A Case of Recurrent Major Cryptogenic Stroke
Harpreet Matharu, Kennedy Aikins, Kumail Rizvi, and Danielle Ford
Background
It is estimated that 30 to 40% of all strokes have no identifiable cause; these are classified as cryptogenic strokes. Often, the unknown nature is secondary to delayed or incomplete investigation of cerebrovascular pathology. At times, strokes are considered truly cryptogenic as extensive stroke workup leads to no identifiable cause or etiology. Acute ischemic strokes in young adults without identifiable risk factors present a diagnostic and therapeutic challenge. Prompt recognition and treatment are critical to optimize outcomes.
Case Presentation
A 32-year-old African American male with a past medical history of a cerebrovascular accident in 2023 at an outside hospital with no residual symptoms presented to the emergency department with a one-day history of left-sided facial droop, dysarthria, and left upper and lower extremity weakness. Initial CT of the brain without contrast showed an area of hypoattenuation in the right temporal lobe without any space-occupying lesion. CT of the neck showed a partially occlusive thrombus in the distal right MCA M1 segment extending into the superior division of the M2 segment with decreased flow in the distal M2 and M3 branches.
As the patient’s initial presentation was within the treatment window for TNK, the patient received TNK. A comprehensive stroke workup, including cardiac monitoring, echocardiography, hypercoagulability panel, vascular imaging, and drug screening, revealed no identifiable etiology or conventional risk factors.
Further imaging with MRI of the head/brain without contrast showed acute small‑volume infarcts in the right insular cortex and posterior frontal lobe, with smaller foci of restricted diffusion involving the right superior and posterior temporal lobe and the left superior cerebellum, without any acute hemorrhage. Bilateral venous Doppler ultrasound did not show any identifiable DVTs.
Lessons Learned / Conclusion
This case underscores the importance of maintaining a high index of suspicion for ischemic stroke in young adults even in the absence of traditional risk factors. It also highlights the need for further investigation into potential underlying mechanisms of cryptogenic stroke in this population.
-

The Rapid Case of Anoxic Brain Injury Secondary to Hyperammonemia
Jacqueline Bekhit, Ngoc Vu, Jiaming Xue, Gabriella David, and Qasim Sajawal
Background: Acute hyperammonemia presents as a toxic state with the clinical presentation as altered consciousness, seizures, and coma. Hyperammonemia disrupts astrocytes osmotic balance via glutamine accumulation, triggering brain edema, inflammation, and apoptosis whom mechanism is closely parallel to hypoxic ischemic injury. This overlap necessitates differentiating metabolic causes from hypoxic etiologies, as timely ammonia clearance therapies can prevent catastrophic outcomes. This case underscores the need for close clinical vigilance and early recognition of severe hyperammonemia
Case Presentation: A 65-year-old woman with metabolic dysfunction-associated steatotic liver disease related cirrhosis complicated by recurrent ascites requiring bimonthly paracentesis presented with abdominal distension and pain. Her most recent paracentesis was two weeks prior in which 5L of ascitic fluids was removed. On admission, she was alert and oriented with a mildly elevated ammonia level of 58 µmol/L. On day 2, 4L of ascitic fluid were removed with concurrent albumin administration. On day 3 in the morning, she was placed on 4L nasal canula for increased work of breathing. Later the same day, patient had a rapid response called for acute respiratory distress and seizure-like activity, and subsequently, transfer to ICU and intubated. Repeat ammonia level obtained during rapid response showed increased to 975 µmol/L. MRI head revealed global anoxic brain injury. After multidisciplinary discussion and a family meeting, the patient was transitioned to comfort measures and expired later on the same day.
Lessons Learned: Catastrophic consequences can occur in “routine” admissions for compensated cirrhotic patients as decompensation can occur rapidly. Close monitoring for early signs of decompensation with prompt actions is necessary to mitigate mortality.
Conclusion: This case illustrates the potential for catastrophic decompensation in cirrhotic patients resulting in global anoxic brain injury in an otherwise compensated cirrhotic setting. The rapid rise of serum ammonia level likely reflects both increase production and impaired clearance. Patients with advanced liver disease, chronic kidney disease, and recurrent ascites may be particularly susceptible to such ammonia elevation and consequent deterioration. Early risk stratification, close monitoring, and prompt escalation of neurocritical care in patients demonstrating early clinical signs of hyperammonemia may be critical in mitigating morbidity and mortality.
-

The Scope Effect: A Quality Improvement Initiative to Enhance Communication, Awareness, and Connection in Family Medicine Residency
Shana-Kay Lambert-Johnson, Amy Nguyen-Pham, and Tasaduq Mir
-

The Unlikely Case of Sporadic Immune Thrombotic Thrombocytopenic Purpura with Refractory and Seizure-like Activity Features: Case Report
Brandon Gremmer and Alain Folefack
Introduction/Background: Thrombotic Thrombocytopenic Purpura (TTP) is a multisystem disease that can lead to multiorgan failure by disseminated mechanical destruction, microangiopathic hemolytic anemia, and thrombocytopenia. Most TTP cases are classified as acquired or hereditary; however, sporadic immune TTP with a refractory episode during the same hospital admission is not well documented in the literature. Furthermore, seizure-like activity during plasma exchange is not a common adverse effect.
Case Presentation: A 35-year-old African American female with no documented medical, surgical, or social history, changes to medications, or lifestyle changes presented with full body fatigue, fever, loss of balance, and confusion. On arrival, labs demonstrated severe thrombocytopenia and anemia with elevation in bilirubin specifically indirect bilirubin, ferritin, lactate dehydrogenase, troponins, and creatinine. TTP was the suspected diagnosis after a peripheral blood smear showed extensive schistocytes. Plasma exchange with Methylprednisolone IV was immediately initiated. During the night on day 2, one seizure-like episode with transient right facial and right sided weakness followed by confusion witnessed. Plasma exchange stopped. On day 6, ADAMTS13 was < 2%. By day 13, labs then showed worsening thrombocytopenia and anemia, plasma exchange restarted. Stable improvement in labs and symptoms on day 19 and the patient was cleared for discharge from the hospital.
Learning points: Most TTP cases are diagnosed as acquired with a definite etiology. However, sporadic immune TTP is considered a diagnosis of exclusion. Regardless, it is extremely important to identify and begin emergent treatment and preferably guided by a hematologist where available. In rare cases of refractory TTP, it is crucial that the patient understands the importance of being followed by outpatient hematology to avoid or manage relapses. Overall, our case report may provide new insights on monitoring the mainstay treatment regimen for adverse effects or refractory symptoms.
-

Too Young for a Broken Heart: STEMI at Twenty
Shana-Kay Lambert-Johnson and Jason Thompson
Background: ST-elevation myocardial infarction (STEMI) is exceptionally rare in young adults, accounting for less than 1% of acute coronary syndromes in individuals younger than 35 years. When it occurs in early adulthood, particularly among women, it introduces diagnostic uncertainty and exposes gaps in post-discharge continuity of care. This case of a 20-year-old female with STEMI highlights the role of primary care in preserving evidence-based therapy while addressing psychosocial determinants of recovery.
Case Presentation: A 20-year-old female presented to her primary care clinic for post-discharge follow-up after hospitalization for an anterior STEMI that began with sudden-onset substernal chest pain radiating to the left arm. Electrocardiography demonstrated anterior ST-segment elevations, and emergent cardiac catheterization revealed an isolated 85% stenosis of the mid left anterior descending artery, treated with percutaneous coronary intervention (PCI) and drug-eluting stent placement. No additional coronary disease or spontaneous coronary artery dissection was identified. Post-infarction echocardiography showed a left ventricular ejection fraction of 40–45% with anterior-apical hypokinesis and grade II diastolic dysfunction. Inpatient evaluation, including lipid panel, hemoglobin A1c, and thyroid-stimulating hormone, was unremarkable. Urine drug screening was positive for marijuana and benzodiazepines but negative for cocaine and methamphetamine. She was discharged on guideline-directed medical therapy, including aspirin, ticagrelor, high-intensity statin therapy, metoprolol succinate, sacubitril/valsartan, spironolactone, and losartan, with a recommendation for 12 months of dual antiplatelet therapy (DAPT). At outpatient follow-up, she was clinically stable but reported impending loss of insurance coverage, limiting ticagrelor affordability to three months. Her body mass index was 42 kg/m², and she had a history of severe depression and anxiety with visible affective distress, declining depression screening. Motivational interviewing was initiated with behavioral health support. Outpatient management expanded to include advanced lipid testing, thrombophilia and autoimmune evaluation, cardiology follow-up, weight management, substance use counseling, medication assistance enrollment, and transition to clopidogrel to maintain DAPT adherence.
Learning Points: STEMI in patients younger than 35 years is uncommon and warrants evaluation beyond traditional atherosclerotic risk factors. Standard inpatient testing may be insufficient, making structured outpatient diagnostic expansion essential. Twelve months of DAPT following acute coronary syndrome with PCI is a Class I guideline recommendation, and failure to address medication affordability and insurance instability increases the risk of premature discontinuation. Cardiac rehabilitation and psychological support are essential components of recovery. This case demonstrates how coordinated outpatient primary care can preserve evidence-based therapy while addressing the clinical and psychosocial consequences of premature myocardial infarction.
-

Tricenarian Seizure Cascade: Uremic Encephalopathy and Suspected Dialysis Disequilibrium
Purva Dahat, Jessica Nguyen, Sara Abuelayyan, and Amnah Andrabi
Introduction Uremic encephalopathy and dialysis disequilibrium syndrome (DDS) are distinct neurologic complications of renal failure that can precipitate seizures. While uremic encephalopathy reflects toxin-mediated metabolic dysfunction, DDS may occur during hemodialysis initiation from rapid osmotic shifts. They are usually described as separate entities, particularly in established CKD. Sequential neurologic events spanning the pre-dialysis period and dialysis initiation in previously undiagnosed renal failure are poorly characterized.
Case presentation A previously healthy African American man in his 30s with no known history of kidney disease presented with new-onset generalized tonic-clonic seizure accompanied by respiratory distress. Initial laboratory testing revealed profound azotemia with severe metabolic derangements consistent with end-stage renal disease (ESRD) physiology. Cross-sectional imaging demonstrated a solitary kidney without prior documented renal evaluation. During the same admission, he was newly diagnosed with HIV. Family history was notable for lupus nephropathy in his father; however, an extensive autoimmune workup in the patient was unrevealing. Neuroimaging excluded acute intracranial hemorrhage, mass lesion, and radiographic evidence of opportunistic infection. In the setting of extreme uremia, the presenting seizure was most consistent with uremic encephalopathy, a recognized neurologic manifestation of advanced renal failure. Hemodialysis was initiated. During an early dialysis session, he developed recurrent seizure with abrupt neurologic deterioration. Given the tight temporal association with dialysis initiation and the markedly elevated baseline azotemia, dialysis disequilibrium syndrome (DDS) was suspected, a complication linked to rapid solute reduction and cerebral edema risk. Dialysis was immediately modified to a slower, staged clearance strategy. No further seizures occurred, and the patient’s neurologic status steadily improved with ongoing renal replacement therapy.
Learning Pearls
1. Severe renal dysfunction with neurologic symptoms constitutes an urgent indication for renal replacement therapy, as encephalopathy and seizures due to uremia are potentially reversible with dialysis.
2. The discovery of a new comorbidity during hospitalization should not narrow the differential prematurely. Clinicians must guard against anchoring bias and continue systematic evaluation of common etiologies.
3. Delayed presentation of advanced disease highlights the importance of routine preventive care, early screening, and timely engagement with the healthcare system to reduce morbidity from potentially modifiable conditions.
Conclusion This case illustrates a clinically important overlap between metabolic encephalopathy and dialysis-related neurologic injury in severe, previously unrecognized end-stage renal disease in the setting of a solitary kidney and concurrent newly identified HIV infection, followed by an intradialytic seizure concerning for dialysis disequilibrium syndrome. The occurrence of both a pre-dialysis seizure attributed to severe uremia and a subsequent intradialytic seizure temporally linked to hemodialysis initiation is infrequently detailed in the literature. This case underscores the importance of early recognition of overlapping metabolic and treatment-related neurologic risk and supports staged, low-efficiency dialysis initiation to mitigate neurologic complications in profoundly azotemic patients.
-

True Love: Heart Says To The Kidneys ‘Don’t Fail Me’
Greeshma Molugu, Srinivasan Rajaganapathy, and Machaiah Madhrira
Introduction: Valvular calcification is an increasingly important cardiac valvular pathology in end-stage renal disease (ESRD) patients, most frequently involving the aortic and mitral valves. The incidence/prevalence of mitral annular calcification in ESRD patients is about 30%, with mitral stenosis occurring in less than 5%. Various predisposing factors for valvular calcification in ESRD patients include age (median age >/= 60 years), hypertension, diabetes, use of calcitriol and calcium-containing phosphate binders, secondary hyperparathyroidism and duration of dialysis (median duration of >/= 5 years). We present a rare case of a young male with ESRD on peritoneal dialysis (PD) for less than two years, who developed severe mitral stenosis requiring mechanical mitral valve replacement (MVR).
Case description: A 30-year-old male with ESRD secondary to hypertension who was on PD for less than two years presented with volume overload and exertional dyspnea. His symptoms did not show significant improvement despite the adjustment of his PD prescription. Transthoracic echocardiography (TTE) revealed an ejection fraction (EF) of 55-60%, mitral annular and valvular calcification with severe mitral stenosis (mitral valve area 1.2 cm2, mean gradient 19mm Hg). TTE performed a year ago showed a similar EF with only mild calcification of the mitral valve without stenosis. Cardiac catheterization ruled out coronary artery disease and confirmed the findings of severe mitral stenosis for which the patient underwent mechanical mitral valve replacement with intraoperative histology confirming the presence of extensive mitral valvular calcification.
Discussion/Conclusion: Cardiac valvular calcification is a strong and independent predictor for all-cause mortality and cardiovascular death in ESRD patients. It is also associated with various complications, including chamber dilation leading to arrhythmias, risk for thrombosis/bleeding, and infective endocarditis. It has been established that the rate of valvular calcification is accelerated in ESRD patients compared with the general population. Calcification can be up to tenfold faster in ESRD patients compared with patients with milder stages of chronic kidney disease (CKD) not undergoing dialysis. Clinical diagnosis based on physical examination can be challenging due to the labile volume status of patients undergoing dialysis. Hence, a high index of suspicion should be applied to perform echocardiography to detect valvular calcification and valvular stenosis, especially in the presence of symptoms. This case report is unique as the development of severe calcific mitral stenosis requiring intervention was in a young male who was on peritoneal dialysis for less than two years. It also highlights the rapid progression of the valvular abnormality, thus emphasizing the importance of early referral to cardiology, and guideline-directed management, including follow-up echocardiograms to reduce mortality and morbidity.
-

Use of Preoperative Chlorhexidine Scrub in Prevention of Groin Surgical Site Infections
Enoch Wong, Pranay Arora, Hunter Knight, Carissa Lucero, and Edic Stephanian
Background: Surgical site infections (SSIs) following groin exposure in vascular surgery are associated with significant morbidity, prolonged hospital length of stay, and increased healthcare costs. The groin is particularly susceptible to infection due to local skin flora and moisture, with studies demonstrating higher infection rates compared to other vascular operative sites (1). Despite standard perioperative infection prevention measures in the operating room, SSI rates following groin exposure remain unacceptably high. This quality improvement (QI) project aimed to reduce groin SSI rates through the implementation of a standardized preoperative chlorhexidine-based scrub protocol.
Methods: A single-center QI initiative was evaluated using a before-and-after study design. The control group consisted of patients who underwent standard preoperative hair clipping and OR prep per facility protocol. 161 adult patients undergoing vascular procedures requiring groin exposure between July 2023 and April 2025 were included in the control group. The intervention consisted of chlorhexidine scrub self-administered by patients to the groin prior to elective outpatient vascular procedures involving groin exposure. Education was provided to patients and clinic staff to ensure protocol adherence. The primary outcome was subsequent OR procedures for groin SSI debridement noted on chart review. Secondary outcomes included groin wound vac placement and microbiology data.
Results: The study included a total of 161 pre-intervention patients with rates of return to OR for groin SSI debridement at 16.1%, higher than previously published studies (2). Post-intervention data collection is ongoing.
Conclusions: Analysis of the pre-intervention cohort demonstrated higher than expected rates of groin SSI requiring operative debridement. There is need for strategies to reduce groin SSI in vascular surgery patients, justifying the implementation of our ongoing pre-operative chlorhexidine scrub initiative. Ongoing monitoring of SSI rates and protocol adherence will better characterize the efficacy of enhanced skin antisepsis protocols for high-risk surgical sites in vascular surgery.
-

White Plaques with High Stakes: A Case of Esophageal Leukoplakia
Boney Lapsiwala, Ritika Sharma, Karthik Kasireddy, Devika Pavuluri, Rupali Prabhukhot, and Amjad Awan
Introduction: Esophageal leukoplakia, also termed esophageal epidermoid metaplasia (EEM), is a rare esophageal epithelial disorder characterized by keratinized squamous plaques on esophagogastroduodenoscopy (EGD). With a prevalence of < 0.5%, it is often incidentally identified during evaluation for nonspecific upper gastrointestinal symptoms. EEM is considered a premalignant condition due to its association with esophageal squamous cell carcinoma (SCC), yet management and surveillance strategies remain undefined.
Case Presentation: A 65-year-old woman with hypothyroidism, hypertension, hyperlipidemia, and remote aplastic anemia treated with bone marrow transplantation 35 years prior presented with chronic cough and progressive dysphagia to solids and liquids. She denied tobacco, alcohol, or illicit drug use. No weight loss, abdominal pain, or blood in stool was noted. CT of the neck with contrast revealed curvilinear mucosal hyperenhancement involving the mid to distal thoracic esophagus without lymphadenopathy. Physical examination and vital signs were unremarkable. EGD revealed a ringed esophagus with diffuse and localized mucosal abnormalities in the mid-esophagus, initially concerning for eosinophilic esophagitis. Histopathology demonstrated low-grade squamous dysplasia on random biopsies (BX) and high-grade squamous dysplasia on targeted mid-esophageal BX. Alcian blue and periodic acid–Schiff stains were negative. Immunohistochemical staining demonstrated increased Ki-67 proliferation index and positive p53 expression. The patient was initiated on proton pump inhibitor therapy. Repeat EGD at four-week follow-up demonstrated extensive white, lacy, scaly mucosa with granulation tissue involving approximately 80% of the esophageal circumference from 24 to 32 cm from the incisors. Repeat biopsies revealed extensive parakeratosis with full-thickness squamous dysplasia, without evidence of invasive malignancy, consistent with EEM. Given the rapid interval progression despite negative biopsies for invasive carcinoma, patient-physician discussion is essential to guide further management and surveillance.
Learning points: EEM is a premalignant squamous lesion with reported progression to SCC in approximately 25%. P53 is the most frequently implicated mutation, with additional alterations reported in PIK3CA, EGFR, MYCN, HRAS, and the TERT promoter. Although causality is unproven, associations with tobacco exposure, including second-hand smoke and alcohol use, have been described. Larger dysplastic lesions may benefit from endoscopic resection or ablative therapies such as radiofrequency ablation or argon plasma coagulation.
Conclusion: EEM is a precursor to SCC, and vigilant recognition is essential for early detection. Management includes addressing the underlying risk factors and focusing on individualised endoscopic surveillance of the area of leukoplakia as well as the surrounding background mucosa.
 by Jasmine M. Silva and Vinay Antin")
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
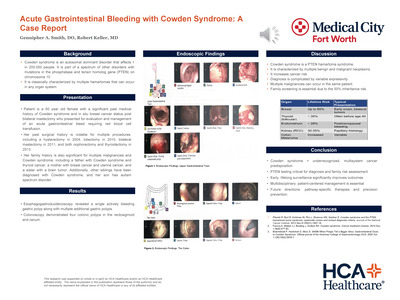{kind=link}
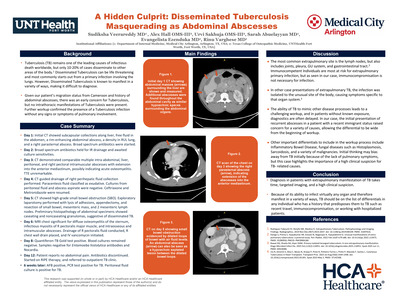{kind=link}
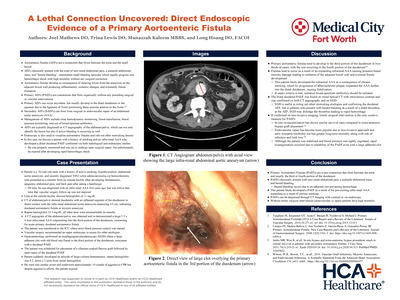{kind=link}
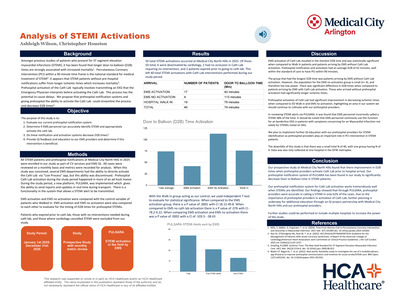{kind=link}
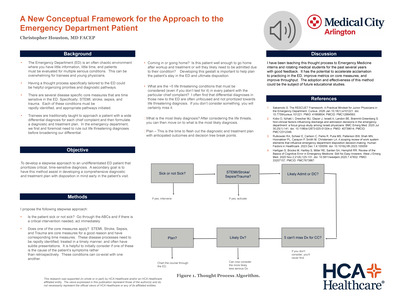{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
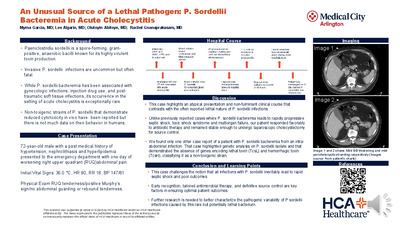{kind=link}
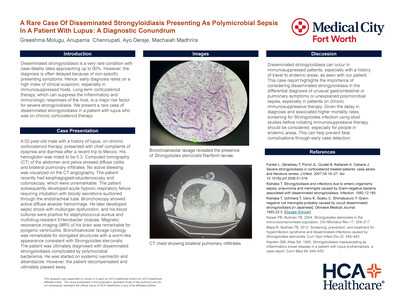{kind=link}
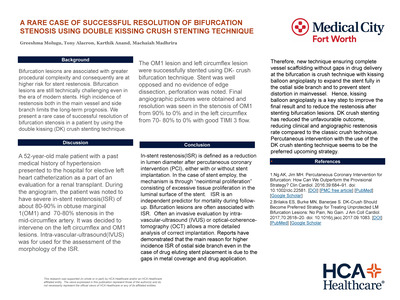{kind=link}
{kind=link}
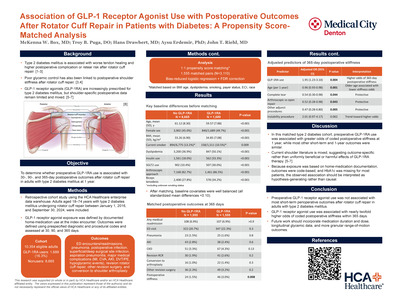{kind=link}
{kind=link}
{kind=link}
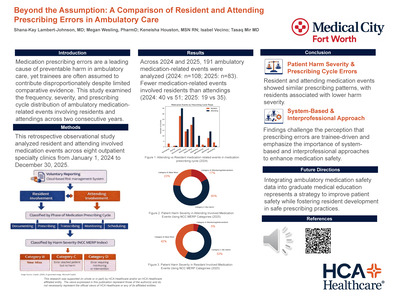{kind=link}
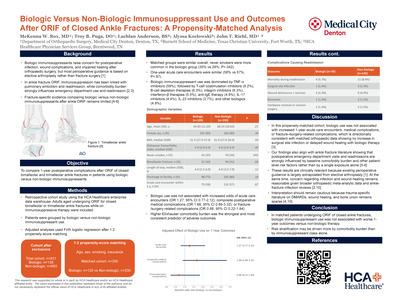{kind=link}
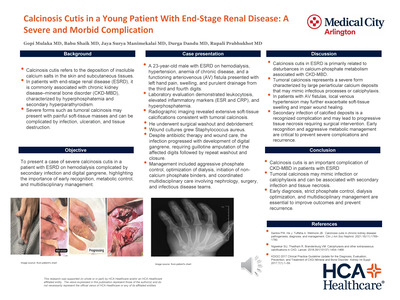{kind=link}
{kind=link}
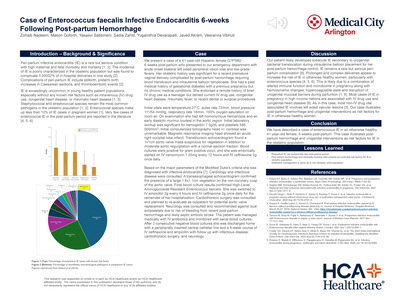{kind=link}
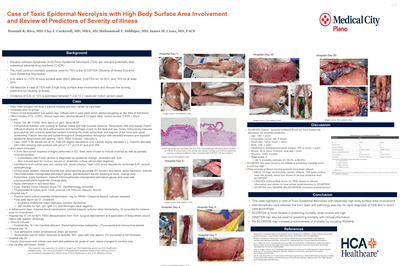{kind=link}
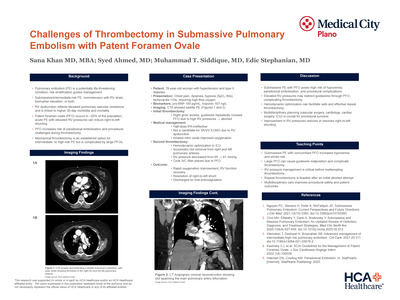{kind=link}
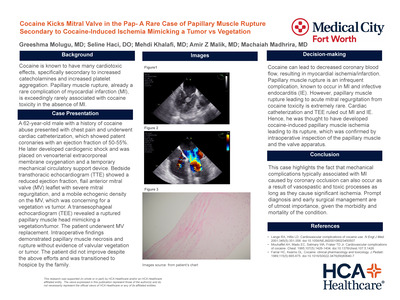{kind=link}
{kind=link}
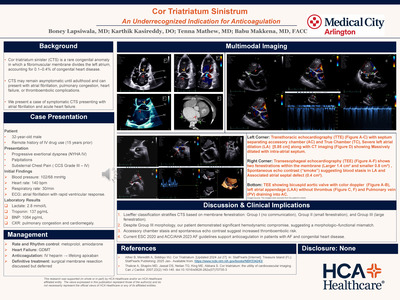{kind=link}
{kind=link}
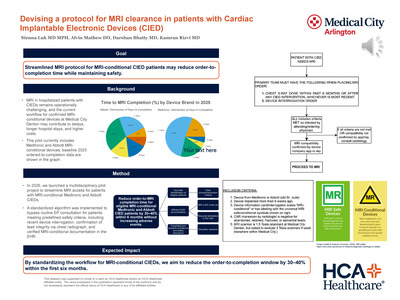{kind=link}
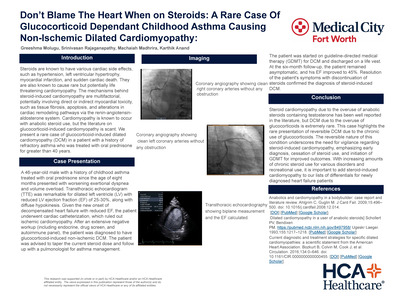{kind=link}
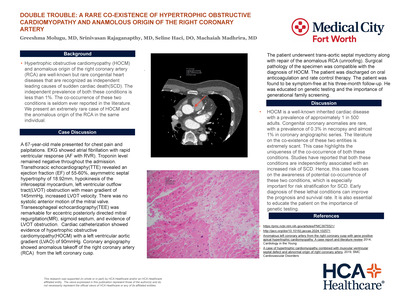{kind=link}
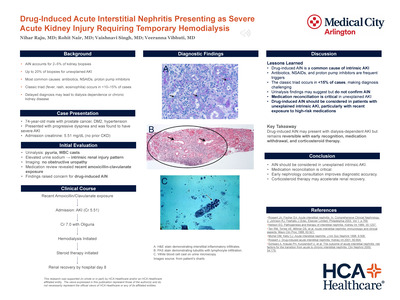{kind=link}
{kind=link}
{kind=link}
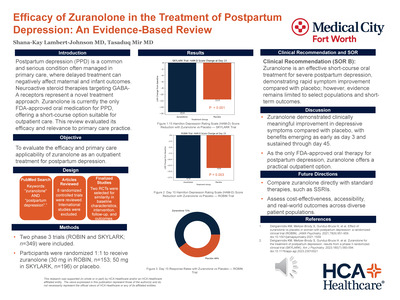{kind=link}
{kind=link}
{kind=link}
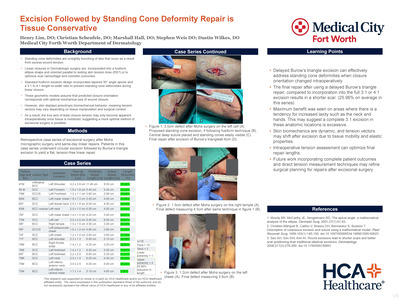{kind=link}
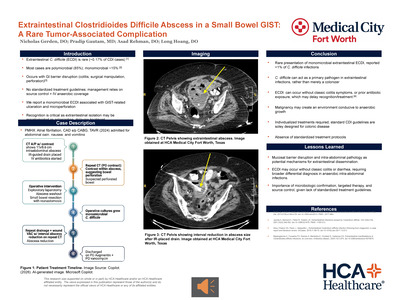{kind=link}
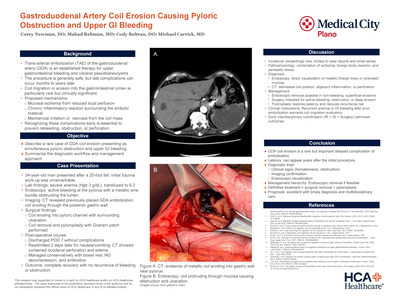{kind=link}
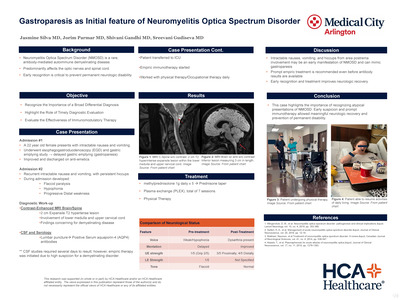{kind=link}
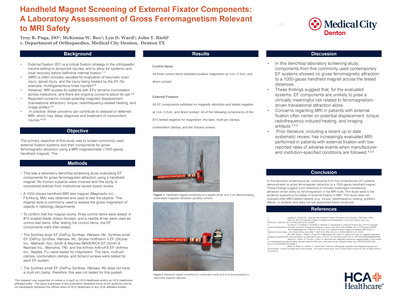{kind=link}
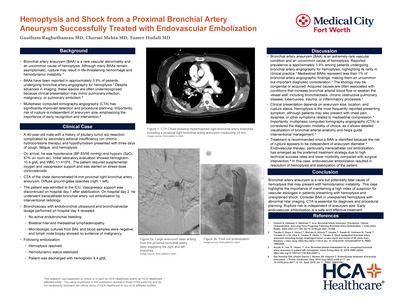{kind=link}
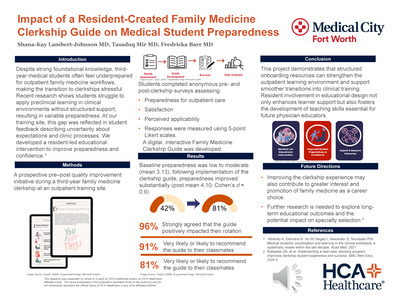{kind=link}
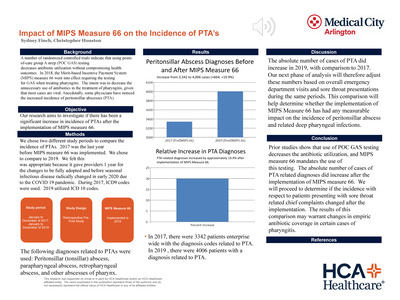{kind=link}
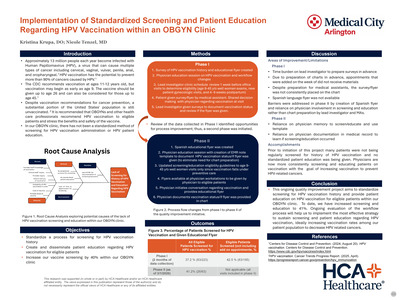{kind=link}
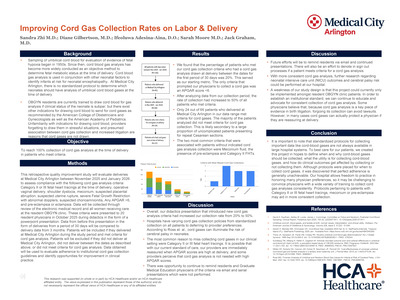{kind=link}
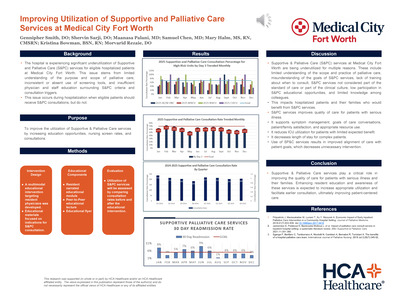{kind=link}
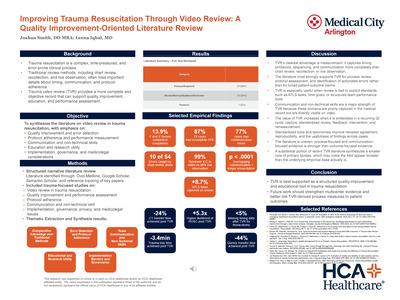{kind=link}
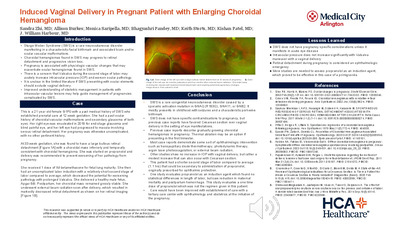{kind=link}
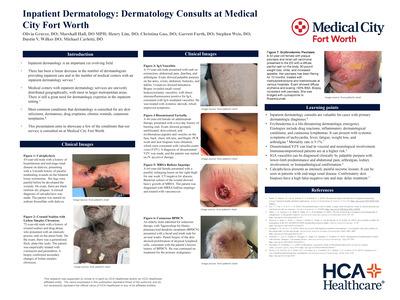{kind=link}
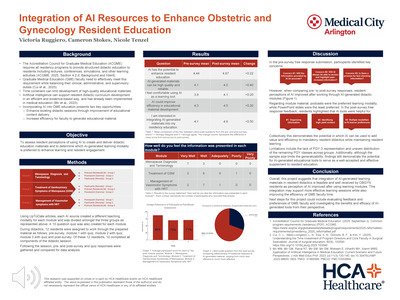{kind=link}
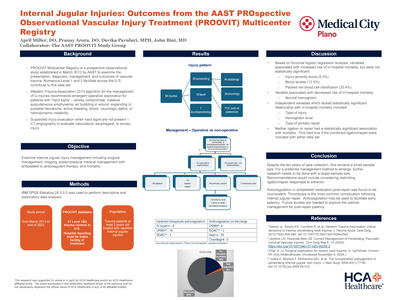{kind=link}
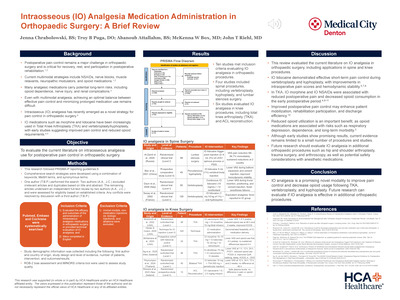{kind=link}
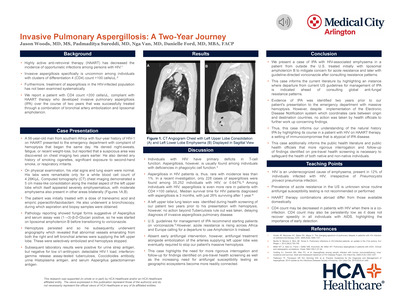{kind=link}
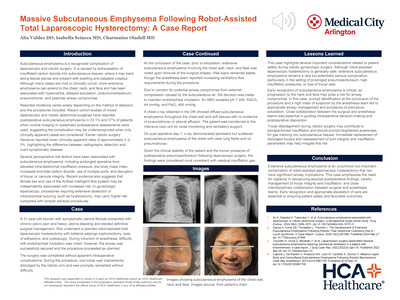{kind=link}
{kind=link}
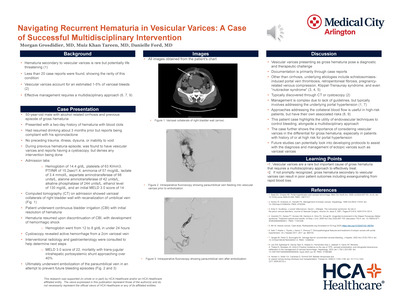{kind=link}
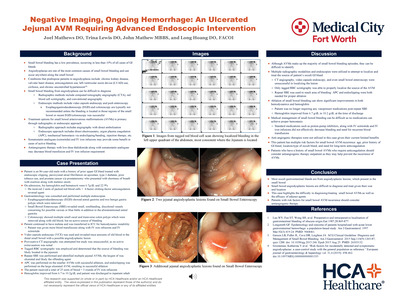{kind=link}
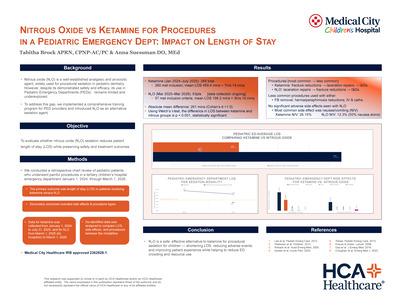{kind=link}
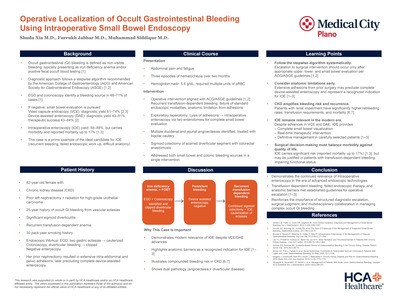{kind=link}
{kind=link}
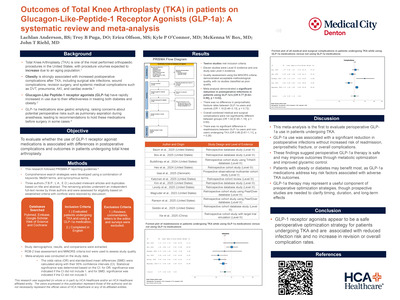{kind=link}
{kind=link}
{kind=link}
{kind=link}
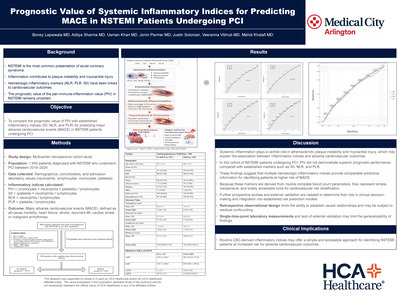{kind=link}
{kind=link}
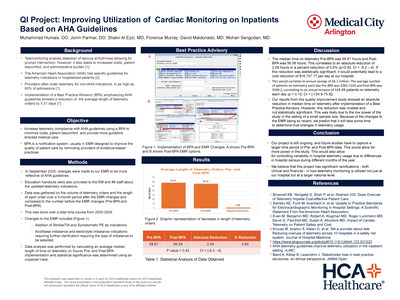{kind=link}
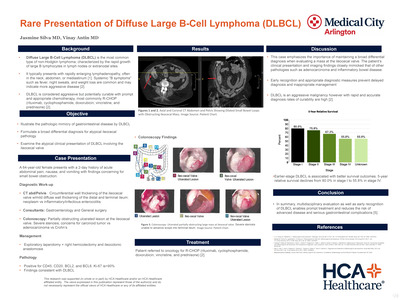{kind=link}
{kind=link}
{kind=link}
{kind=link}
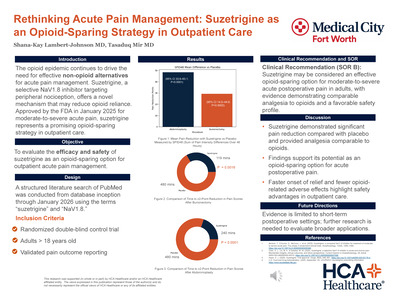{kind=link}
{kind=link}
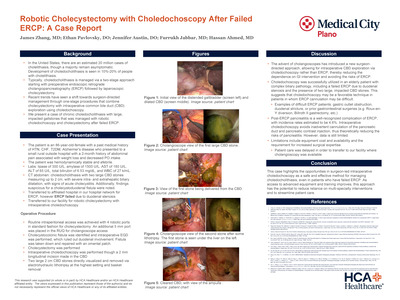{kind=link}
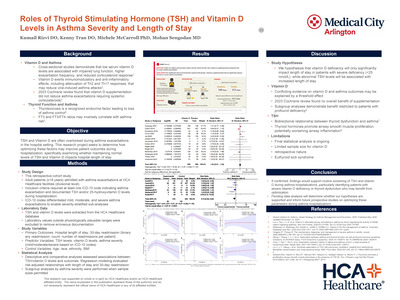{kind=link}
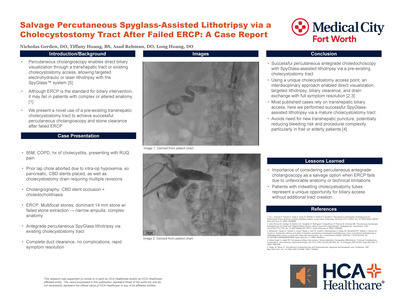{kind=link}
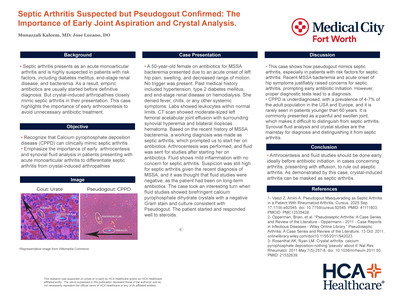{kind=link}
{kind=link}
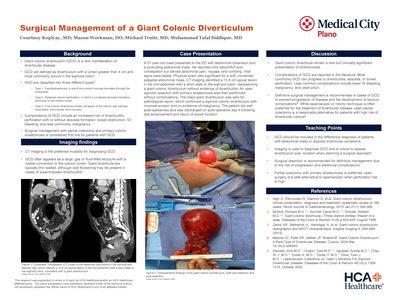{kind=link}
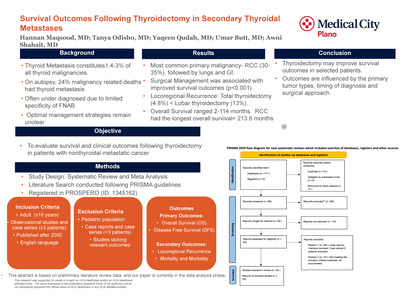{kind=link}
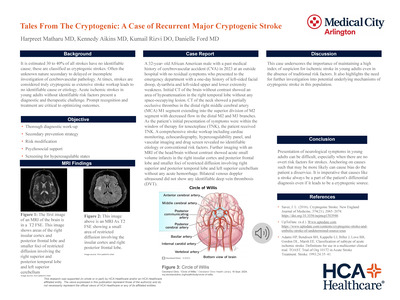{kind=link}
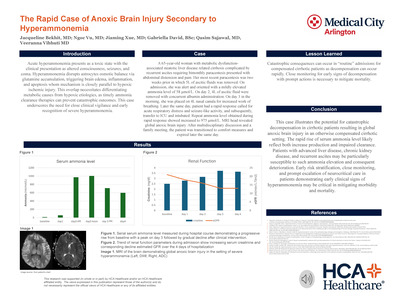{kind=link}
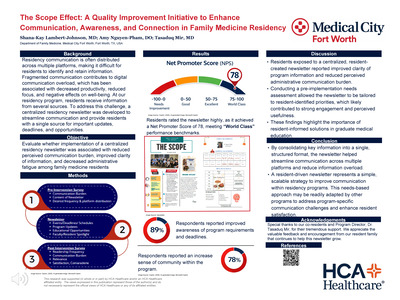{kind=link}
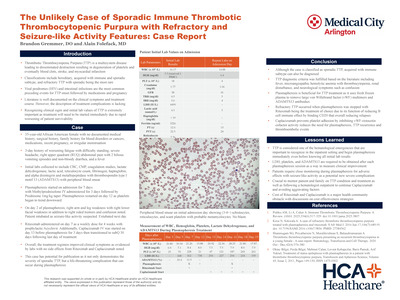{kind=link}
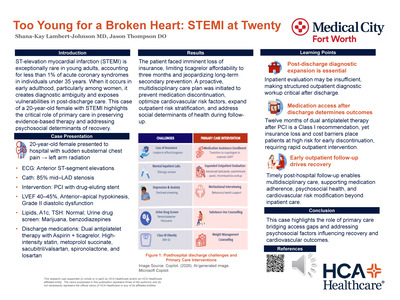{kind=link}
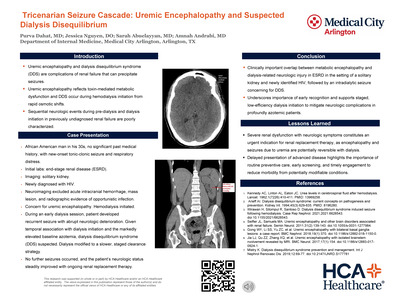{kind=link}
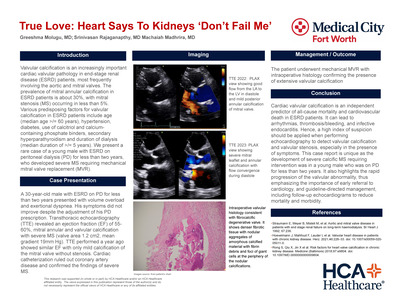{kind=link}
{kind=link}
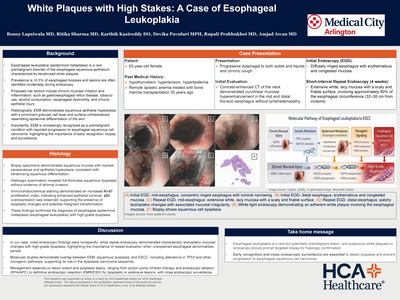{kind=link}