


-

A Case of Aggressive Diffuse B-Cell Lymphoma in Brain: Diagnostic Pitfalls
Jaya Surya Manimekalai Krishnamurthi
-

A Case of Median Raphe Cysts in 8-year-old Male
Christina Guo, Marshall Hall, Garrett Furth, Henry Lim, Olivia Gruver, Dustin Wilkes, and Stephen E. Weis
Background: The median raphe cyst is a rare, benign, congenital condition characterized by small, fluid-filled cysts that develop along the ventral midline of male external genitalia. These cysts are usually asymptomatic during infancy and childhood but tend to grow in size as the patient grows. These can become cosmetically concerning or symptomatic due to swelling, irritation, and discomfort. They may also present social and psychological stress to patients and families. We present a case of median raphe cysts in an 8-year-old male.
Case Presentation: An 8-year-old male without a prior medical history who presented to dermatology for penile lesions. He exhibited these penile lesions since birth. The lesions had grown in size. The lesions were initially asymptomatic, but he had begun to scratch at these lesions due to irritation. He denied pain, drainage, and bleeding. His family was concerned that these lesions would affect the patient’s sexual function in the future and that these lesions might continue to grow larger. The patient had also undergone testing several times for sexually transmitted diseases. On physical exam, there were thin, skin-colored, shiny papules along the midline ventral aspect of the penile shaft. Based on the classic clinical presentation, a diagnosis of median raphe cysts was established. Reassurance was provided that these were benign lesions. If there were symptomatic or cosmetic concerns, surgical management with urology was recommended
Conclusion: Median raphe cysts are rare congenital lesions that can cause significant physical and emotional stress to patients. In clinical practice, these cysts must be differentiated from other, more common penile lesions. This condition can be diagnosed based on clinical information, but biopsy can aid in confirmation. It is important for clinicians to recognize these lesions in order to reassure patients and families about the benign nature of the lesions and limit unnecessary testing. While these lesions are benign and typically asymptomatic, they can become a source of pain, are susceptible to secondary infection, and can be a significant cosmetic or sexual concern. Surgical removal is a safe and effective way to remove these lesions when symptomatic.
-

Acute Gastrointestinal Bleeding Associated with Cowden Syndrome: A Case Report
Gennipher A. Smith and Robert Keller
-

A Hidden Culprit: Disseminated Tuberculosis Masquerading as Abdominal Abscesses
Sudiksha Veerareddy, Alex Hall, Urvi Sakhuja, Sarah Abuelayyan, Evangelista Ezenduka, and Rinu Varghese
Introduction: Tuberculosis (TB) is an insidious pulmonary infection that is most prevalent in developing countries. Primary TB may also become latent after initial infection and remain dormant in the body until the patient becomes immunocompromised. The infection will then resume and can become disseminated, moving hematogenously and through the lymphatics to other areas of the body. Disseminated TB is known to manifest in a variety of ways, making it difficult to diagnose.
Case Presentation: A 28-year-old- male patient presented to Medical City Arlington with complaints of left lower quadrant abdominal pain. He immigrated from Cameroon 4 years prior. Initial CT imaging showed a rim-enhancing abdominal abscess, sub-capsular collections along the liver, and free fluid in the abdomen. CT angiogram revealed an 8 mm density in the right upper lung lobe, adjacent edema and enlargement of the right pectoralis major muscle, and right parasternal abscess with areas of cortical destruction of the body of the sternum. On day 3, repeat CT demonstrated comparable multiple intra-abdominal, liver, peritoneal, and right pectoral intramuscular abscesses with extension into the anterior mediastinum. On day 4, CT-guided drainage of the right perihepatic fluid collection was performed. Paracentesis fluid was classified as exudative and cultures showed no organisms. On day 5, imaging showed high-grade small bowel obstruction, likely secondary to multiple abdominal abscesses. Exploratory laparotomy was performed with extensive lysis of adhesions and abdominal organ and lymph node resections. Preliminary histopathology of abdominal specimens showed caseating and noncaseating granulomas, suggestive of disseminated TB. The following day, MRI was significant for diffuse osteomyelitis of the sternum with infectious myositis of the right pectoralis major muscle. Thus, a drainage of the right pectoralis fluid collection was conducted. On day 8, a Quantiferon-TB Gold test was shown to be positive, suggesting disseminated TB. On day 12, the patient was initiated on RIPE therapy. After a few weeks, peritoneal fluid AFB PCR and culture were positive for TB.
Learning Points: Because of its ability to infect virtually any organ and therefore manifest in a variety of ways, TB should be on the list of differentials in any individual with a history that predisposes them to TB such as recent travel or immunocompromisation. The ability of TB to mimic other disease processes leads to a challenging workup. This case highlights the importance of a high clinical suspicion as well as an awareness for these niche cases of extrapulmonary presentation.
-

A Lethal Connection Uncovered: Direct Endoscopic Evidence of a Primary Aortoenteric Fistula
Joel Mathews, Trina Lewis, Munazzah Kaleem, and Long Hoang
BACKGROUND: Primary Aortoenteric Fistulas (PAEFs) are a rare condition that occurs when the native aorta develops an abnormal connection with the gastrointestinal lumen. PAEFs tend to develop within the duodenum, specifically the distal region of the third part of the duodenum, which is retroperitoneal and is anterior to the aorta. Duodenal PAEFs can be difficult to diagnose and are often lethal, given their non-specific presenting symptoms and rapid progression to hemorrhagic shock.
CASE PRESENTATION: This case focuses on a 70-year-old male with a history of T4N2 colon adenocarcinoma with hemicolectomy, active smoking, and abdominal aortic aneurysm (AAA) who was transferred for evaluation of hematemesis. CT of abdomen/pelvis at the outside hospital showed duodenitis with an inflamed segment of the duodenum in direct contact with the infra-renal abdominal aortic aneurysm measuring 4.6cm, concerning for possible duodenal aortoenteric fistula. Repeat CT imaging on admission re-demonstrated a large 5.2 x 4.4cm infra-renal AAA outpouching into the third portion of the duodenum, concerning for acute primary duodenal aortoenteric fistula. The patient was transferred to the Medical ICU unit, and strict blood pressure control with IV nicardipine drip. Due to uncertainty regarding the possibility of a primary duodenal aortoenteric fistula, a CT Angiogram of the abdomen/pelvis was obtained and confirmed 5.2 x 4.4cm infra-renal AAA outpouching into the third portion of the duodenum with free air inferior to the duodenal sweep, indicating a contained duodenal aortoenteric fistula. Vascular surgery evaluated the patient and recommended endoscopy to assess for other etiologies. EGD was performed, and a large adherent clot with old blood was found in the third portion of the duodenum, consistent with a duodenal PAEF. Vascular surgery re-evaluated the patient afterwards and planned for open repair; however, the patient developed massive-volume hematemesis and went into cardiac arrest. Despite aggressive resuscitation efforts, the patient expired later that day.
CONCLUSION: This case highlights the difficulty in managing Duodenal PAEFs and the importance of early diagnosis and surgical intervention to maximize patient survival, as delayed interventions often lead to lethal consequences as a result of rapid exsanguination.
-

Analysis of STEMI Activations
Ashleigh Wilson and Christopher Houston
Background Prior studies of ST-segment elevation myocardial infarctions (STEMI) presentations have shown that longer door-to-balloon (D2B) times are associated with increased mortality. Percutaneous Coronary Intervention (PCI) within 90-minutes is standard. It appears that STEMI patients without prehospital notifications have longer ischemic times. Prehospital activation of cathlab involves EKG transmission that the Emergency Physician interprets before activating cathlab, which has the potential to cause delays. We propose that prehospital notification and prehospital having the ability to activate cathlab could decrease D2B times.
Study aims:
- Evaluate current prehospital notification system.
- Assess EMS accuracy in STEMI identification and cathlab activation.
- Does prehospital notification decrease D2B times?
- Provide QI education to EMS providers.
Methods All STEMI and prehospital notifications at Medical City North Hills were enrolled prospectively in our study as part of CV services and EMS QI. Cases were reviewed monthly, and metrics were recorded. At study onset, several EMS departments had the ability to activate cathlab via “Live-Process,” but this was discontinued. Prehospital cathlab activation during the study period was more improvised. During the study, a new platform, PULSARA, was implemented, that can send updates in real-time and includes a STEMI alert function.
Results From 1/1/2025 - 12/31/2025, there were 50 STEMI activations. 6 were deactivated by cardiology, 2 had no occlusion, and 2 expired. Of the 40 cases with intervention, the average D2B time was 74 minutes. 26 arrived by EMS; 21 received interventions with an average D2B time of 55 minutes. EMS activated cathlab 22 times; with 17 interventions with an average D2B time of 42 minutes. 4 cases arrived by EMS without prehospital activation with average D2B time of 113 minutes. 24 activations walked in resulting in 19 interventions with an average D2B time of 76 minutes. Overall, there were 34 STEMI alerts sent via PULSARA, 13 of which did not meet STEMI criteria, and cathlab wasn’t activated. Conclusion The shortest D2B times were prehospital activation by EMS, and the longest were those arriving by EMS without prehospital activation. The N for this last group was small and may not be statistically significant, but clinically it was. Of the STEMI alerts sent via PULSARA for cathlab activation, 38% were incorrectly identified. It is likely that some of these alerts were due to concerning EKGs. Going forward, we plan to use the PULSARA system to activate cathlab and will provide education to our EMS partners.
-

A New Conceptual Framework for the Approach to the Emergency Department Patient
Christopher Houston
Background
The Emergency Department (ED) is an often chaotic environment where you have little information, little time, and must evaluate for multiple serious conditions. This can be overwhelming for trainees and young physicians. Having a thought process specifically tailored to the ED could be helpful organizing priorities and diagnostic pathways. There are several disease specific core measures that are time sensitive in the ED. Specifically; STEMI, stroke, sepsis, and trauma. Each of these conditions must be rapidly identified, and appropriate pathways initiated.
Trainees are traditionally taught to approach a patient with a wide differential diagnosis for each chief complaint and then formulate a diagnostic and treatment plan. In the emergency department, we first and foremost need to rule out life threatening diagnoses before broadening our differential.
Method
I propose and teach the following stepwise approach.
-Is the patient sick or not sick? Go through the ABCs and if there is a critical intervention needed, act immediately.
-Does one of the core measures apply? STEMI, Stroke, Sepsis, and Trauma are core measures for a good reason and have corresponding time measures. These disease processes need to be rapidly evaluated, treated in a timely manner, and often have subtle presentations. It is helpful to initially consider if one of these is the cause of the patient’s symptoms rather than retrospectively. These conditions can co-exist with one another.
-Coming in or going home? Is this patient well enough to go home, or will they ultimately need to be admitted due to their condition? Developing this gestalt is important to help plan the patient’s stay in the ED and ultimate disposition.
-What are the ~5 life threatening conditions that must be considered (even if you don’t test for it) in every patient with the chief complaint? I often find that differential diagnoses in those new to the ED are often unfocused. If you don’t consider something, you will certainly miss it.
-What is the most likely, actual diagnosis? After considering the life threats, you can then move on to what is the most likely diagnosis.
Conclusion
I have been teaching this thought process to Emergency Medicine interns and rotating medical students for the past several years with good feedback. It has the potential to accelerate acclamation to practicing in the ED, improve metrics on core measures, and improve throughput. The adoption and effectiveness of this method could be the subject of future educational studies.
-

A Not So Typical Case of Alcoholic Pancreatitis
Wendy Phillips, Kaleem Munazzah, Asad Rehman, and Robert Keller
BACKGROUND Acute pancreatitis (AP) has become one of the leading gastrointestinal diagnoses resulting in inpatient hospitalization¹. AP is diagnosed by meeting two of three criteria: characteristic clinical presentation, biochemical evidence (elevated lipase or amylase levels), and imaging findings with pancreatic inflammation. Gallstones and heavy alcohol use account for most cases (40%–70% and 25%–35%, respectively). Hypertriglyceride induced AP (HTG-AP) accounts for only about 7-10% of AP cases³ and often tends to present in younger, male, obese, patients with a higher rate of diabetes¹. Below we present a unique case of a coinciding alcoholic and HTG - AP in an otherwise healthy female and discuss the importance of early diagnosis and appropriate treatment.
CASE DESCRIPTION The patient is a 56-year-old woman with a history of alcohol use disorder and scoliosis who presented with epigastric pain, nausea, and vomiting. She reported drinking twelve 12-oz beers daily and had one prior hospitalization for alcohol-related pancreatitis earlier this year. Lipase on admission was 632 U/L, and abdominal MRI showed peripancreatic edema consistent with AP. Her alcohol level was elevated which further supported alcoholic pancreatitis. To complete the AP workup, triglyceride (TG) level was collected and found to be markedly elevated at 2740 mg/dL. The patient was promptly admitted and started on an insulin drip with 87% TG reduction within 24 hours. She was then transitioned to fenofibrate and discharged on orlistat, fenofibrate, and dietary modifications.
DISCUSSION Patients with HTG-AP are at higher risk for severe disease progression and complications, including respiratory and circulatory failure, compared with other etiologies⁴. While plasmapheresis was traditionally the mainstay of treatment, recent evidence supports early insulin therapy, which achieves similar clinical outcomes with fewer adverse events and lower costs⁵. After TGs are reduced to < 1,000 mg/dL, patients should be started on triglyceride-lowering therapy and counseled on lifestyle modifications. After discharge, patients should follow closely with a provider to monitor triglyceride levels, as recurrence occurs in up to about 20% of cases².
-

Antibody-Mediated Allograft Rejection 23 Years After Heart Transplant
Jorim Parmar, Boney Lapsiwala, Devika Adusumilli, Sienna Luk, Nguyen Dung, Song Li, and Kamala Tamirisa
INTRODUCTION: Orthotopic heart transplantation (OHT) remains the gold standard treatment for patients with advanced heart failure refractory to optimal medical and device-based therapies. Despite advances in perioperative management, immunosuppressive regimens, and long-term surveillance protocols, graft rejection remains a major determinant of post-transplant morbidity and mortality [1]. We report a case, representing one of the longest documented intervals in literature, of suspected antibody-mediated rejection (AMR) occurring 23 years after heart transplantation in which conventional endomyocardial biopsy (EMB) could not be successfully performed. This case highlights the diagnostic uncertainty associated with very late AMR and underscores the potential role of clinical presentation, immunologic biomarkers, and advanced imaging modalities in guiding diagnosis and management when histopathologic confirmation is not feasible.
CASE PRESENTATION: A 73-year-old man with a history of OHT presented for evaluation of suspected antibody-mediated rejection (AMR), reflected by elevated class II donor-specific antibodies (DSA) and a Donor-derived cell-free DNA (dd-cfDNA) assay score of 0.4. He had no prior history of rejection or graft dysfunction. His immunosuppression regimen included sirolimus and mycophenolate mofetil. EMB was attempted and unsuccessful twice. Transthoracic echography and cardiac MRI revealed moderate left ventricular dysfunction and severely dilated atria. MRI showed marked LA enlargement (9.2 x 9.4 cm) and moderate-to-severe RA dilation, with prolonged T2 signals (59 msec) (Figures). Left heart catherization revealed a 40% stenosis of the left anterior descending artery, consistent with Grade 1 CAV. He was treated for presumed AMR with plasmapheresis, IV immunoglobulin, high-dose corticosteroids, anti-thymocyte globulin, and adjustment of immunosuppression regimen.
DISCUSSION: AMR is a feared complication of solid organ transplantation [2]. Etiology is likely multifactorial, involving postoperative structural changes and possible subclinical immunologic injury leading to fibrosis and impaired atrial compliance. The interactions between humoral and cellular immunity in chronic allograft dysfunction is complicated making clinicians unable to depend on a single marker as a sole indicator of rejection [3]. EMB is the gold-standard but they are invasive, carry risks, and can be done a limited amount of times [4,5]. Cardiac MRI is emerging as a comprehensive assessment of function, morphology, and tissue characterization without these risks [6].
CONCLUSION: Patients with long-term OHT may develop chronic graft dysfunction secondary to AMR despite being asymptomatic, showing the importance of regular surveillance. Cardiac MRI may detect dysfunction missed by echocardiography. Our findings underscore the importance of integrating clinical presentation, advanced imaging, and emerging biomarkers to support diagnosis and management when EMB is not feasible.
-

An Unusual Case of Genetic Dilated Cardiomyopathy Unmasked by COVID-19 Infection
Greeshma Molugu, Daniel McMahan, Seline Haci, Giridhar Mundluru, and Machaiah Madhrira
Introduction: Titin (TTN) mutations are a well-known cause of dilated cardiomyopathy (DCM), occurring in approximately 25% of familial cases of idiopathic DCM and 18% of sporadic cases. Recognition and referral for genetic testing remains underutilized but has important prognostication and helps the patient better understand the disease transmission. This case report stresses the importance of a complete evaluation for genetic causes of DCM.
Case Presentation: A 21-year-old male who was adopted as an infant was hospitalized with COVID-19 infection and diagnosed with non-ischemic cardiomyopathy with an initial left ventricular ejection fraction (EF) of 10%. He was assumed to have DCM secondary to his viral infection and was discharged on guideline-directed medical therapy (GDMT) without any further workup. However, he was lost to follow-up, and two years later, he presented in cardiogenic shock leading to pulseless electrical activity (PEA) arrest. His EF then was 5-10% with global hypokinesis, dilation of all four chambers, and severely reduced right ventricular (RV) function. He was placed on venoarterial extracorporeal membrane oxygenation (VA ECMO) with an Impella 5.5. Cardiac magnetic resonance imaging (MRI) showed four-chamber cardiomegaly without contrast uptake, no evidence of arrhythmogenic RV dysplasia, no focal wall motion abnormality, and no late gadolinium enhancement. Genetic testing was positive for an autosomal dominant heterozygous TTN mutation. The patient was decannulated and discharged on GDMT and a LifeVest. His EF at the three-month follow-up improved to 50-55%.
Discussion: Genetic DCM is often underdiagnosed due to false assumptions or incomplete workup. Our patient went years without a complete workup before his diagnosis was understood. Also, our patient was adopted, but the studies have shown the importance of screening family members for early identification of familial DCM and improved survival rates. Gene-environment interactions play a vital role in the development of DCM. Studies have shown that TTN gene mutations can predispose individuals to specific types of cardiomyopathy when combined with environmental factors. This was likely seen in our patient, as both presentations occurred following a COVID-19 infection. Hence, a complete workup at the time of diagnosis will aid in patient education on their disease, familial transmission rates, and the importance of medical compliance and follow-up.
-

An Unusual Culprit Behind a Massive Pulmonary Embolism: Atypical May-Thurner Syndrome from Iliac Artery Aneurysm
Boney Lapsiwala, Jiaming Xue, Mayank Singh, Sai Krishan Reddy Dronadula, Sadia Zahid, and Mian Yousef
Background: Venous thromboembolism (VTE) is a major cause of global morbidity and mortality. May-Thurner syndrome (MTS) is an iliofemoral venous compression syndrome caused by extrinsic compression of the left common iliac vein (LCIV), classically by the right common iliac artery at the level of the fifth lumbar vertebra. Although the estimated anatomic prevalence ranges from 18-49%, only 2-5% of cases are diagnosed during evaluation for lower-extremity deep vein thrombosis (DVT). Clinical manifestations range from asymptomatic venous compression to unilateral leg swelling, venous insufficiency, and acute iliofemoral DVT, with pulmonary embolism (PE) reported infrequently.
Case presentation: A 75-year-old man with hypertension, hyperlipidemia, rheumatoid arthritis, and a remote postoperative DVT presented with acute-onset dyspnea. CT pulmonary angiography revealed a massive, occlusive PE involving the right main and left pulmonary arteries with evidence of right heart strain. Lower-extremity venous duplex USG showed extensive left iliofemoral DVT. Subsequent CT angiography of the abdomen and pelvis identified aneurysmal dilation of the LCI artery with associated mural thrombus, resulting in extrinsic compression of the adjacent LCIV, consistent with an atypical variant of MTS. Given a high Pulmonary Embolism Severity Index score (115), the patient underwent percutaneous mechanical aspiration thrombectomy for PE. On hospital day three, staged left lower-extremity mechanical aspiration thrombectomy was performed, followed by angioplasty and venous stenting with a 16 × 150 mm Abre venous stent. Post-dilation with a 16 × 40 mm balloon and intravascular ultrasound (IVUS) confirmed full stent expansion, appropriate wall apposition, and restoration of luminal flow. The patient was discharged on apixaban for at least six months and clopidogrel for two to three months. At follow-up, he subsequently underwent elective endovascular repair of the left common iliac artery aneurysm to prevent further progression.
Learning points: MTS should be considered in patients with recurrent venous thromboembolism despite minimal or absent symptoms. Diagnosis relies on multimodality imaging, with venous duplex USG as the initial screening tool and venography with IVUS as the reference standard for definitive anatomic assessment. Management strategies are guided by symptom burden and thrombotic complications. Asymptomatic or mildly symptomatic patients are typically managed conservatively, whereas symptomatic disease warrants an individualized endovascular approach. Anticoagulation following venous stenting should be tailored to thrombotic risk factors and overall clinical presentation.
Conclusion: MTS may represent a provoked cause of pulmonary embolism despite negative hematologic evaluation, warranting timely recognition and early management.
-

An Unusual Source of a Lethal Pathogen: Paeniclostridium sordellii Bacteremia in Acute Cholecystitis
Myrna Garcia, Leena Algarin, Olutoyin Abitoye, and Rachel Gnanaprakasam
Paeniclostridium sordellii is a spore-forming, gram-positive, anaerobic bacilli known for its highly virulent toxin production, often leading to fulminant sepsis and shock. It is most commonly associated with gynecologic infections and necrotizing soft tissue infections associated with intravenous drug use. However, reports of P. sordellii bacteremia in the setting of gall bladder infections are quite rare. This case report highlights an unusual presentation of P. sordellii infection with bloodstream infection originating from acute cholecystitis, demonstrating a non-fulminant clinical course and successful treatment with ceftriaxone.
-

A Rare Case of Disseminated Strongyloidiasis Causing Polymicrobial Sepsis in a Patient with Lupus: A Diagnostic Conundrum
Greeshma Molugu, Anupama Chennupati, Ayo Dereje, and Machaiah Madhrira
Introduction: Disseminated strongyloidiasis is a very rare condition with case-fatality rates approaching 90%. However, the diagnosis is often delayed because of nonspecific presenting symptoms. Early diagnosis relies on a high index of clinical suspicion, especially in immunocompromised hosts. Long-term corticosteroid therapy, leading to some suppression of inflammatory and immunologic responses, is a well-known risk factor for severe strongyloidiasis.
Case presentation: A 52-year-old male with a past medical history of lupus on chronic corticosteroid therapy presented with chief complaints of dyspnea and diarrhea. He has a recent history of travel to Mexico. Hemoglobin was 5.3. CTAP with contrast showed diffuse colitis and bilateral pulmonary infiltrates. CTA showed no evidence of active bleed. Had recent upper and lower GI scopes which were negative. Patient developed acute hypoxic respiratory failure requiring intubation with bloody secretions suctioned through the ET tube. Had bronchoscopy which showed active alveolar hemorrhage. He later developed septic shock with multiorgan dysfunction. Blood cultures were positive for staphylococcus aureus and multidrug resistant enterobacter cloace. His MRI Brain was remarkable for pyogenic ventriculitis. BAL cytology was remarkable for elongated structures with worm like appearance consistent with Strongylides stercoralis. The patient was finally diagnosed to have disseminated strongyloides complicated by polymicrobial bacteremia. He was started on iv ivermectin and albendazole, however, the patient decompensated and passed away.
Discussion: Severe strongyloidiasis is a risk in every corticosteroid-treated patient who has traveled to a soil-infested country, as seen with our patient. This case highlights the importance of considering disseminated strongyloidiasis in the differential diagnosis of unusual gastrointestinal or pulmonary symptoms or unexplained polymicrobial sepsis, especially in patients on chronic immunosuppressive therapy. Hence, screening for Strongyloides infection using stool studies before initiating immunosuppressive therapy should be considered, especially in endemic areas. This can help prevent fatal complications through early case detection.
-

A Rare Case of Successful Resolution of Bifurcation Stenosis Using Double Kissing Crush Stenting Technique
Greeshma Molugu, Tony Alacron, Karthik Anand, and Machaiah Madhrira
Introduction: Bifurcation lesions are associated with greater procedural complexity and consequently are at higher risk for stent restenosis. Bifurcation lesions are still technically challenging even in the era of modern stents. High incidence of restenosis both in the main vesseI and side branch Iimits the Iong-term prognosis. We present a rare case of successful resolution of bifurcation stenosis in a patient by using the double kissing (DK) crush stenting technique.
Case Description: A 52-year-old male patient with a past medical history of hypertension presented to the hospital for elective left heart catheterization as a part of an evaluation for a renal transplant. During the angiogram, the patient was noted to have severe in-stent restenosis(ISR) of about 80-90% in obtuse marginal 1(OM1) and 70-80% stenosis in the mid-circumflex artery. It was decided to intervene on the left circumflex and OM1 lesions. Intra-vascular-ultrasound(IVUS) was for used for the assessment of the morphology of the ISR. The OM1 lesion and left circumflex lesion were successfully stented using DK- crush bifurcation technique. Stent was well opposed and no evidence of edge dissection, perforation was noted. Final angiographic pictures were obtained and resolution was seen in the stenosis of OM1 from 90% to 0% and in the left circumflex from 70- 80% to 0% with good TIMI 3 flow.
Conclusion: In-stent restenosis(ISR) is defined as a reduction in lumen diameter after percutaneous coronary intervention (PCI), either with or without stent implantation. In the case of stent employ, the mechanism is through “neointimal proliferation” consisting of excessive tissue proliferation in the luminal surface of the stent. ISR is an independent predictor for mortality during follow-up. Bifurcation lesions are often associated with ISR. Often an invasive evaluation by intra-vascular-ultrasound (IVUS) or optical-coherence-tomography (OCT) allows a more detailed analysis of correct implantation. Reports have demonstrated that the main reason for higher incidence ISR of ostial side branch even in the case of drug eluting stent placement is due to the gaps in metal coverage and drug application. Therefore, new technique ensuring complete vessel scaffolding without gaps in drug delivery at the bifurcation is crush technique with kissing balloon angioplasty to expand the stent fully in the ostiaI side branch and to prevent stent distortion in mainvessel.Hence, kissing balloon angioplasty is a key step to improve the final result and to reduce the restenosis after stenting bifurcation Iesions. DK crush stenting has reduced the unfavourable outcome, reducing clinical and angiographic restenosis rate compared to the classic crush technique. Percutaneous intervention with the use of the DK crush stenting technique seems to be the preferred upcoming strategy.
-

Ashwagandha-Associated Liver Injury: A Systematic Literature Review
David Teplitsky, Jacob Sebaugh, Danielle Ford, and Rashid Syed
Background: Ashwagandha (Withania somnifera), an herb with origins in Ayurvedic medicine, has recently grown in global popularity due to its reported stress- and anxiety-relieving properties. While generally regarded as safe, emerging cases in medical literature have raised concern for its ability to cause drug- or herb-induced liver injury (DILI/HILI). As use of this supplement rises, it is particularly important to characterize ashwagandha’s potential hepatotoxicity.
Methods: Cases of ashwagandha-induced liver injury were collected by accessing PubMed, Europe PMC, Google Scholar, and the HCA Healthcare Library and searching combinations of the terms “liver” or “hepatic” and one of the following names for the herb: “Withania”, “ashwagandha”, “Indian ginseng”, or “winter cherry”. Each case report or case series was screened to ensure ashwagandha was the likely causative agent of liver injury, and that no other potentially hepatotoxic supplement was being taken by the patients.
Results: Thirty-seven cases were identified from literature review. The patients had an average age (SD, range) of 41 (16, 19-75) and a male:female ratio of 22:15. Seventy-eight percent of patients presented with jaundice and 51% with pruritis, and approximately 30% with nausea/vomiting, fatigue/malaise, or abdominal pain. Peak values of pertinent labwork revealed an average peak AST of 377 (521, 47-2500), average peak ALT 562 (846, 34-3692), average peak ALP 251 (159, 59-893), average peak total bilirubin 14.3 (8.4, 2-31.5), and average peak INR of 1.7 (1.5, 0.9-6.2). The type of liver injury was 49% hepatocellular, 24% mixed, 19% cholestatic, and 8% unable to be calculated due to missing labwork. Three reported cases resulted in death, 1 required transplantation, and the rest either resolved spontaneously or with steroids, ursodeoxycholic acid, cholestyramine, hydroxyzine, or N-acetylcysteine.
Conclusion: The majority of reported cases of ashwagandha-related liver injury reveal a hepatocellular liver injury with no notable relation with sex or age. While most cases resolved spontaneously or with symptomatic treatment, several cases of ashwagandha-induced liver injury have resulted in death or transplantation; thus, the potential hepatotoxic effects of ashwagandha must be considered when evaluating cases of supplement-induced liver injury.
-

Association of GLP-1 Receptor Agonist Use with Postoperative Outcomes After Rotator Cuff Repair in Patients with Diabetes: A Propensity Score–Matched Analysis
McKenna W. Box, Troy B. Puga, Hans Drawbert, Aysu Erdemir, and John T. Riehl
Background Diabetes impairs tendon healing after rotator cuff repair (RCR), with early postoperative poor glycemic control linked to a higher failure risk in studies. GLP-1 receptor agonists (GLP-1RAs) are increasingly used for glycemic control. Preclinical studies indicate that GLP-1RA may benefit rotator cuff healing through anti-inflammatory mechanisms as well. However, real-world data on the effects of GLP-1RAs on RCR outcomes remain incompletely understood.
Methods We conducted a retrospective cohort study using an institutional dataset (01/01/2016 to 09/30/2024) of adults aged 18-74 years with type 2 diabetes who underwent RCR. GLP-1RA exposure was established by home medication lists. Patients with autoimmune diseases, type 1 diabetes, chronic kidney disease, myocardial infarction, associated shoulder-girdle fractures, or shoulder arthroplasty were excluded. Outcome measures were assessed up to 1 year after surgery and included ED visits, pneumonia, revision shoulder surgery for rotator cuff re-tear or conversion to arthroplasty, and postoperative stiffness. Propensity scores were estimated using logistic regression, and patients were matched 1:1 to patients with diabetes not on a GLP-1RA. Post-match balance was assessed using standardized mean differences. Post-matching outcomes were evaluated using bias-reduced logistic regression for rare events, with cluster-robust standard errors within matched pairs. The Benjamini-Hochberg false discovery rate adjustment was applied to all modeled outcomes.
Results Among 10,354 eligible patients, 1,689 (16.3%) were users of GLP-1RA. After application of exclusion criteria, 1,555 GLP-1RA users were matched with 1,555 non-users (N = 3,110). After multiplicity adjustment, GLP-1RA use was associated with higher odds of postoperative stiffness (OR 1.953, 95% CI 1.232-3.096; adjusted P = .048). No significant associations were observed for ED readmissions (30/90/365 days), pneumonia readmissions (90/365 days), revision RCR or conversion to arthroplasty (all adjusted P > .30). Other outcomes were not analyzable due to low event counts.
Conclusions In this propensity score-matched cohort of diabetic patients undergoing RCR, GLP-1RA use was not associated with differences in most short-term perioperative outcomes. A statistically significant association with postoperative stiffness within 1 year was observed. Overall, postoperative events were uncommon, and the finding should be interpreted as associative and hypothesis-generating for future studies.
-

A Storm at Both Ends: Hypertensive Emergency Unmaksing C3-Dominant Glomerulonephritis
Karthik Kasireddy, Boney Lapsiwala, Marisha Sharma, Rupali Prabhukhot, and Victor Canela
Background: C3 glomerulopathy (C3G) encompasses a group of diseases that result from abnormalities in the alternative pathway of complement regulation, and has been defined by C3 only or C3-dominant immunofluorescence staining seen on renal biopsy. C3G includes C3 glomerulonephritis (C3GN) and dense deposit disease (DDD); the latter of which is characterized ultra-structurally by the presence of highly osmiophilic intramembranous deposits. Both C3GN and DDD often present with a membranoproliferative pattern of glomerular injury, a finding that can also be seen in thrombotic microangiopathy (TMA). Most common causes include infection, autoimmune and monoclonal gammopathy.
Case presentation: A 70-year-old man with hypertension, prediabetes, obesity, and stage 4 chronic kidney disease presented with headache and generalized weakness and was found to have a blood pressure of 250/118 mmHg, consistent with hypertensive emergency. One week earlier, he had been treated with corticosteroids for a generalized rash. Despite blood pressure stabilization, he developed rapidly progressive renal failure requiring intensive care admission, intubation, and renal replacement therapy. Renal biopsy demonstrated dominant C3 deposition (3+) with coarse granular staining along glomerular capillary loops and mesangium, consistent with C3-dominant glomerulonephritis. Complment C3 was 19, rest unremarkable. Autoimmune, infectious, and monoclonal gammopathy evaluations were negative. He was discharged on optimized antihypertensive therapy. He had repeat admission for generalized maculopapular rash. currently managed with immunosuppression with plans for complement-directed therapy.
Lesson learned: C3Gn can masked with underlying kidney disease. Renal biopsy is main diagnostic tool. In addition, immunological/biochemical evidence of complement involvement should be sought by measuring plasma levels of C3, C4, FH, FI, FB, and soluble C5b9 complexes, and by screening autoantibodies (anti-FH, anti-FB, C3Nef, C4Nef, C5Nef). There is great interest and an apparently increasing role of complement inhibition (i.e., off-label utilization of C5 convertase inhibitors such as eculizumab or other novel complement blocking agents like iptacopan). Many patients will be dialysis dependent in 5-year period, suggesting poor prognosis despite optimal treatment.
Conclusion: C3-dominant glomerulonephritis may present as hypertensive emergency and be masked by underlying chronic kidney disease. Early renal biopsy and complement evaluation are critical to guide prognosis and emerging complement-targeted therapy.
-

Automated Adjudication of Cardiogenic Shock from Unstructured Clinical Notes Using an Open-Source Large Language Model
Devika Adusumilli, Luke Taylor, Claudius Mahr, and Song Li
Background Automated adjudication of cardiogenic shock (CS) from unstructured clinical documentation can facilitate clinical case finding and research trial/registry enrollment. While Large Language Models (LLMs) hold considerable promise, commercial cloud-based solutions raise data privacy and cost concerns. We assessed the performance of an open-source, locally run LLM for the adjudication of CS from unstructured progress notes.
Methods Patients from a 22-hospital healthcare system from 2021 to 2024 were identified using ICD-10 codes to form an enriched CS evaluation cohort with a ~1:1 case/non-case ratio. We selected gpt-oss-20b, an open-source LLM capable of running locally on a consumer-grade computer, and tested it without task-specific fine tuning. A total of 105 de-identified cardiology progress notes from distinct patients were independently reviewed by two physicians and the LLM to determine whether the patient had CS or not. Inter-rater agreement was assessed pairwise among reviewers.
Results Inter-reviewer agreement for CS classification between the two physicians was 90% (94/105 notes). Agreement between the LLM and two physicians were 79% and 82%, respectively, in the whole cohort. In a consensus subset (n = 94) where both physicians agreed, the LLM achieved 84% agreement with the human consensus. Among these cases, physicians identified CS in 44 (47%) patients, whereas the LLM classified 49 (52%) as having CS, indicating a slight over-estimation.
Conclusions An open-source, locally run LLM without fine-tuning demonstrated strong concordance with human consensus in identifying CS from unstructured clinical notes. This approach offers a scalable, privacy-safe, and cost-effective alternative to manual adjudication for clinical and research case finding and enrollment.
-

Beyond the Assumption: A Comparison of Resident and Attending Prescribing Errors in Ambulatory Care
Shana-Kay Lambert-Johnson, Megan Wesling, Keneisha Houston, Isabel Vecino, and Tasaduq Mir
BACKGROUND: Medication prescribing errors remain a leading cause of preventable patient harm in ambulatory care. This study examined whether the severity, frequency, and distribution of medication prescribing errors differ between residents and attendings in outpatient settings to inform graduate medical education (GME) and system-level medication safety strategies.
METHODS: This retrospective observational study was conducted across a multi-specialty ambulatory care network. Ambulatory medication-related events involving residents and attendings occurring between January 1 and December 31, 2025, were identified through voluntary reporting in a cloud-based risk management system. Events were categorized by prescriber role and classified using the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) patient harm index and by stage of the medication prescribing cycle. Event frequency, patient harm severity, and distribution across prescribing cycle stages were compared using descriptive statistics and Fisher’s exact test.
RESULTS: A total of 83 ambulatory medication-related events were analyzed, involving attendings (35) and residents (19), with other events involving staff and other clinical operational factors. Most events in both groups reached the patient without harm (Category C). Among attending-involved events, 16.7% required monitoring or intervention (Category D) and 2.8% resulted in temporary harm (Category E), compared with 5.3% of resident-involved events requiring monitoring (Category D) and no resident-associated harm (Categories E–I). Overall, events requiring monitoring or harm (Category D or higher) were more frequent among attending-involved events (19.4% vs 5.3%), with no severe or permanent harm observed. No events in either group resulted in severe harm or death (Categories F–I). Medication-related events occurred across all phases of the prescribing cycle, most frequently during scheduling, documenting, prescribing, and transcribing, with similar clustering across clinician roles.
CONCLUSIONS: Resident and attending-involved ambulatory medication events demonstrated comparable harm profiles and similar distributions across prescribing cycle phases, with no severe or permanent patient harm identified. These findings challenge the perception that prescribing errors are primarily trainee-driven and underscore the importance of system-level and interprofessional medication safety interventions in ambulatory care. Integrating medication safety education with workflow-focused improvements may enhance patient safety while advancing GME across all levels of clinical training.
-

Biologic Versus Non-Biologic Immunosuppressant Use and Outcomes After ORIF of Closed Ankle Fractures: A Propensity-Matched Analysis
McKenna W. Box, Troy B. Puga, Lachlan Anderson, Alyssa Kozlowski, and John T. Riehl
Background: The effect of biologic immunosuppressant therapy on postoperative outcomes following ankle fracture open reduction and internal fixation (ORIF) remains unclear, and concerns regarding infection and impaired healing often influence perioperative decision-making. We hypothesized that biologic immunosuppressant use would be associated with higher rates of postoperative complications following ORIF of closed ankle fractures compared with non-biologic immunosuppressant therapy.
Methods: We conducted a retrospective cohort study using a multi-hospital administrative dataset (2017-2025) to identify adult patients undergoing ORIF for closed bimalleolar or trimalleolar ankle fractures who were prescribed immunosuppressive therapy. Patients were categorized based on biologic versus non-biologic immunosuppressant use. A 1:2 propensity score match was performed based on age, sex, smoking status, insurance type, and diabetes. Outcomes included acute care encounters (ACE) within 1 year (defined as emergency department encounters or hospital admission), postoperative medical complications, and fracturerelated complications. Firth logistic regression was used for adjusted analyses.
Results: After matching, 350 patients were included (biologic, n=120; non-biologic, n=230), with balanced baseline characteristics. One-year acute care encounter rates were similar (58% biologic vs 57% non-biologic, P=.87). Rates of thromboembolic events, surgical site infection, wound complications, malunion, nonunion, delayed union, and revision surgery were low and comparable between groups. In adjusted analyses, biologic immunosuppressant use was not associated with significantly increased odds of ACE (OR 1.27, 95% CI 0.77– 2.12; P=.40), composite postoperative medical complications (OR 1.68, 95% CI 0.89–3.32; P=.12), or fracture-/surgery-related complications (OR 0.68, 95% CI 0.22–1.84; P=.50). Across all models, higher comorbidity burden, as measured by the Elixhauser Comorbidity Index, was the strongest and most consistent predictor of adverse outcomes.
Conclusion: Biologic immunosuppressant use was not associated with increased postoperative risk following ORIF of closed ankle fractures compared with non-biologic immunosuppressant therapy. Overall comorbidity burden, rather than immunosuppressant class, appears to drive postoperative outcomes. These findings support perioperative risk stratification based on global health status rather than medication class alone.
-

Calcinosis Cutis in a Young Patient With End-Stage Renal Disease: A Severe and Morbid Complication
Gopi Mulaka, Babu Shaik, Jaya Surya Manimekalai, Durga Dandu, and Rupali Prabhukhot
BACKGROUND/ INTRODUCTION: Calcinosis cutis is a rare but serious complication of end-stage renal disease (ESRD), often related to disordered calcium–phosphate metabolism. It can lead to significant morbidity, recurrent infections, and challenging management decisions.
CASE PRESENTATION: We present a 23-year-old male with ESRD on hemodialysis, hypertension, anemia of chronic disease, and a left upper extremity arteriovenous fistula who developed progressive pain, swelling, and purulent drainage involving the left third and fourth digits. Imaging revealed extensive soft tissue calcifications consistent with calcinosis cutis. His hospital course was complicated by recurrent infections, osteomyelitis, and gangrene despite antibiotic therapy and wound care, ultimately requiring multiple surgical debridements and amputations.
The patient underwent serial washouts, debridement, and digit amputations in the setting of ongoing infection. Management emphasized multidisciplinary collaboration, optimization of dialysis, aggressive phosphate control, non-calcium phosphate binders, and infectious disease management. Despite these measures, disease progression highlighted the aggressive nature of calcinosis cutis in ESRD.
DISCUSSION: Calcinosis cutis in ESRD is a complication of CKD–mineral bone disorder, driven by hyperphosphatemia and secondary/tertiary hyperparathyroidism. This case is unique due to severe, recurrent tumoral calcinosis in a 23-year-old, causing vascular compromise and pain despite hemodialysis. Current focus emphasizes early recognition and prevention through phosphate control, dialysis optimization, and management of refractory hyperparathyroidism.
TEACHING / LEARNING POINTS:
- Calcinosis cutis in ESRD is a manifestation of CKD–mineral bone disorder, driven primarily by hyperphosphatemia, elevated calcium–phosphate product, and secondary or tertiary hyperparathyroidism.
- Tumoral calcinosis can mimic infection or calciphylaxis, presenting with pain, swelling, erythema, and skin breakdown; secondary infection is common and must be actively excluded.
- AV fistula–related venous hypertension can exacerbate limb swelling and delay healing, confounding clinical assessment of infection and ischemia.
- Management requires a multidisciplinary approach, including nephrology, surgery, and infectious disease, with emphasis on preventing recurrence rather than repeated surgical intervention.
-
, Two Failures Drive Suboptimal VTE Prevention: Quality Improvement by Jorim Parmar, Shakir Al-Ezzi, Anvi Manduva, Muhammad Suleman, Fahed Alsayed, and Debra Medsker")
Cardiac Step-Down Unit (CSU), Two Failures Drive Suboptimal VTE Prevention: Quality Improvement
Jorim Parmar, Shakir Al-Ezzi, Anvi Manduva, Muhammad Suleman, Fahed Alsayed, and Debra Medsker
BACKGROUND: In the Cardiac Step-down Unit (CSU), two failures drive suboptimal VTE prevention: (1). over-ordering of SCDs in patients unlikely to benefit and (2). < 10% documented application when SCDs are truly indicated. Baseline data indicates that curbing over-ordering alone would reduce recorded non-compliance by >50%, revealing a clear opportunity for system redesign.
METHODS: To integrate the updated “3 Bucket” Risk Model assessment into the computerized physician order entry (CPOE) in order to delineate the prophylaxis for a given patient population. Once the manual risk assessment proves to be viable in increasing compliance, we can propose having the tool adopted into the CPOE system. Root Cause Analysis revealed that lack of standardized VTE risk stratification leads to inconsistent ordering practices – some patients receive unnecessary SCDs while others who need them are missed. In addition, nursing compliance with SCD application and documentation is poor, in part due to unclear prioritization and workflow barriers. To address these issues, we propose to implement the updated “3 Bucket” Risk Model as a standardized assessment tool. To address this, we propose that the “3 Bucket” VTE Risk Model will be embedded into the computerized physician order entry (CPOE) system. This integration ensures that appropriate prophylaxis (chemical vs. mechanical) is selected at the time of order entry, which should reduce unnecessary SCD use and improve compliance with indicated devices.
RESULTS: Overuse measure: % of patients with unnecessary SCD orders (patients already appropriately receiving chemical prophylaxis or low risk). Underuse measure (compliance): % of patients with indicated SCD orders who did not have devices applied and documented. In the 3 months prior to the project, compliance with initiated SCD use is < 10%. This poses a dual problem: (1) unnecessary SCD orders add cost and workload without benefit, and (2) underuse of SCDs in patients contraindicated for chemical prophylaxis places high-risk patients at avoidable risk for VTE.
CONCLUSION: Lack of standardized risk stratification leads to both over-ordering of SCDs in low-risk patients or those already on chemical prophylaxis. When SCDs are indicated (e.g. chemical prophylaxis contraindicated), nursing compliance with device application/documentation is < 10%.
-

Case of Enterococcus faecalis Infective Endocarditis 6-weeks Following Post-partum Hemorrhage
Zohaib Nadeem, Mason Goforth, Yasasvi Sabbineni, Sadia Zahid, Yugandhra Devarapalli, Javed Akram, and Veeranna Vibhuti
Peri-partum infective endocarditis (IE) is a rare but serious condition with high maternal and fetal morbidity and mortality. IE is exceedingly uncommon in young healthy patients, especially without any known risk factors such as intravenous (IV) drug use, congenital heart disease, or rheumatic heart disease. IE is estimated to complicate 0.00002% of in-hospital deliveries. Similar to the general population, staphylococcal and streptococcal species remain the most common pathogens in obstetric patients. Enterococcal species make up less than 10% of IE cases in pregnant women. Very few cases of enterococcal IE in the post-partum period are reported in the literature. We describe a case of a 41-year-old female G7P5M2 with Enterococcus faecalis infective endocarditis 6 weeks following post-partum hemorrhage which was managed with intrauterine balloon pump. She initially presented to the emergency department with acute onset bilateral left sided peripheral vision loss and low-grade fevers. Initial vitals were within normal range. On examination she had left homonymous hemianopia and an early diastolic murmur loudest in the aortic region. Magnetic resonance imaging head showed an acute right occipital lobe infarct. Transthoracic echocardiogram found a 1x1cm aortic valve mass suspicious for vegetation in addition to moderate aortic regurgitation with a normal ejection fraction, which was confirmed by transesophageal echocardiogram. Blood cultures were positive for gram positive cocci, and she was empirically started on IV vancomycin and IV ceftriaxone. Based on the major parameters of the Modified Duke’s criteria she was diagnosed with infective endocarditis. Final blood culture results confirmed High-Level Aminoglycoside Resistant Enterococcus faecalis. She was switched to IV ampicillin and IV ceftriaxone for the remainder of her hospitalization. Cardiothoracic surgery was consulted and planned to re-evaluate outpatient for potential aortic valve replacement. After 2 consecutive negative blood cultures she was discharged home with a peripherally inserted central catheter line and a 6-week course of IV ceftriaxone and ampicillin with follow up with infectious disease, cardiothoracic surgery, and neurology. This case illustrates post-partum hemorrhage and urogenital interventions as risk factors for IE in the obstetric population.
-

Case of Toxic Epidermal Necrolysis with High Body Surface Area Involvement and Review of Predictors of Severity of Illness
Hannah R. Riva, Clay J. Cockerell, Muhammad T. Siddique, and James M. Cross
BACKGROUND: Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) are rare and potentially fatal cutaneous adverse drug reactions. The most common mortality predictor used for TEN is the SCORTEN (Severity-of-Illness Score for Toxic Epidermal Necrolysis). Various scoring systems have been used and are being developed for predicting mortality and guiding treatment in SJS/TEN. We describe a case of TEN with a high body surface area involvement and discuss the scoring predictors for severity of illness.
CASE PRESENTATION: A 63-year-old male was transferred to our burn center for a suspected diagnosis of SJS/TEN. He was intubated prior to arrival. He had a recent hospitalization within the past month and underwent a toe amputation. In the prior week he developed a diffuse generalized rash which started sloughing, and he was brought into an outside hospital. On exam, heart rate was tachycardic. There was conjunctival injection with crusting at eyelids and nasal and oral mucosal erosions. There was diffuse erythema on the face with erosions and hemorrhagic crusts on the face and lips. Dusky red/purpuric macules and patches with wrinkled detached centers were overlying the lower extremities and the majority of the torso and upper extremities with flaccid vesicles and bullae throughout. Desquamation was found throughout with denuded erosions and adjacent epidermal detachment with peeling. Over 90% of body surface area was involved. Nikolsky’s sign was positive. Skin punch biopsies confirmed the diagnosis of TEN. SCORTEN score was 5. The patient was admitted to the burn unit and started on intravenous immunoglobulin. Despite ongoing treatment and supportive care, after 20 days the patient was transferred to inpatient hospice care due to worsening status, with death resulting on day 24 after initial hospital admission.
LESSONS LEARNED: This case highlights a case of Toxic Epidermal Necrolysis with especially high body surface area involvement. SCORTEN is more reliable in predicting mortality when scores are high. SCORTEN has been shown to be more reliable than ABCD-10 (Age, bicarbonate, cancer, dialysis, 10% body surface area risk model) in predicting mortality. Clinical Risk Score for TEN (CRISTEN) can also be used for predicting mortality with clinical information. Re-SCORTEN may increase predictiveness of mortality.
CONCLUSION: Understanding the various severity-of-illness scores for SJS/TEN will help dermatologists and providers in burn centers understand how these scoring systems can predict mortality and guide treatment.
-

Challenges of Thrombectomy in Submassive Pulmonary Embolism with Patent Foramen Ovale
Sana Khan, Syed Ahmed, Muhammad T. Siddique, and Edic Stephanian
BACKGROUND/ INTRODUCTION: Submassive, or intermediate-risk, pulmonary embolism (PE) is defined by preserved systemic blood pressure with evidence of right ventricular (RV) strain. The presence of a patent foramen ovale (PFO) in this setting significantly increases the risk of hypoxemia, paradoxical embolization, and procedural complications during catheter-based interventions. Mechanical thrombectomy has become an important treatment option for selected patients with intermediate- to high-risk PE; however, experience in patients with concomitant large PFOs remains limited.
CASE PRESENTATION: A 78-year-old woman presented with acute dyspnea, hypoxemia, and chest pain and was found to have a saddle PE with severe RV dilation and biomarker elevation. She was transferred for mechanical thrombectomy but the initial procedure was aborted after repeated guidewire passage through a large PFO into the left atrium, preventing safe access to the pulmonary arteries. In the intensive care unit, half-dose systemic thrombolysis was administered without clinical or radiographic improvement. Due to persistent hypoxemia and severe RV dysfunction, a multidisciplinary discussion involving vascular surgery, cardiology, cardiac surgery, and critical care resulted in a planned repeat thrombectomy with cardiac surgery on standby. During the second attempt, RV access was achieved, and extensive thrombus was removed from both pulmonary arteries using a mechanical thrombectomy system. RV pressures improved significantly following thrombectomy. A temporary IVC filter was placed to mitigate the risk of paradoxical embolization. The patient rapidly improved after intervention, was weaned off oxygen within 24 hours, and demonstrated progressive recovery of RV function. Follow-up echocardiography showed resolution of right-to-left shunting across the PFO. She was discharged to acute rehabilitation on oral anticoagulation.
DISCUSSION: This case highlights the unique challenges of managing submassive PE in the presence of a large PFO, including catheter malposition due to elevated RV pressures and increased risk of systemic embolization. It demonstrates that repeat mechanical thrombectomy may be safe and effective following an aborted initial attempt when performed with multidisciplinary planning and surgical backup. Recognition of intracardiac shunts and their hemodynamic implications is critical when planning interventional PE therapies.
TEACHING / LEARNING POINTS:
- Submassive PE with concomitant PFO is a high-risk combination that increases the likelihood of hypoxemia, stroke, and hemodynamic compromise.
- Large PFOs with markedly elevated RV pressures can redirect guidewires into the left atrium during thrombectomy attempts, preventing access to the pulmonary arteries.
- Mechanical thrombectomy may still be feasible after an aborted initial attempt, particularly after hemodynamic optimization or procedural modification.
- Multidisciplinary coordination among vascular surgery, cardiology, cardiac surgery, and critical care teams is essential in complex PE cases.
- Reduction of RV pressures after successful thrombectomy can decrease or eliminate right-to-left shunting across a PFO.
-

Cocaine Kicks Mitral Valve in the Pap- A Rare Case of Papillary Muscle Rupture Secondary to Cocaine-Induced Ischemia Mimicking a Tumor vs Vegetation
Greeshma Molugu, Seline Haci, Mehdi Khalafi, Amir Z. Malik, and Machaiah Madhrira
Background: Cocaine is known to have many cardiotoxic effects, specifically secondary to increased sympathetic output from the increased catecholamines, calcium modulation, and increased platelet aggregation. This can cumulatively cause suppression of myocardial contractility and decreased coronary blood flow, resulting in arrhythmias, myocardial ischemia, or even infarction. Papillary muscle rupture, already a rare complication of myocardial infarction (MI), is exceedingly rarely associated with cocaine toxicity in the absence of MI. Also, acute mitral regurgitation(MR) due to papillary muscle rupture from cocaine-induced ischemia remains exceedingly rare. We present a second-ever reported case of papillary muscle rupture secondary to cocaine-induced ischemia in the absence of MI.
Case Description: A 62-year-old male with a past medical history of cocaine abuse who presented with chest pain, underwent a left heart catheterization, which showed patent coronary arteries with an ejection fraction (EF) of 50-55%. He later developed cardiogenic shock with flash pulmonary edema requiring intubation and was placed on VA ECMO and an Impella 5.5. Bedside transthoracic echocardiogram (TTE) showed a reduced EF, flail anterior mitral valve (MV) leaflet with severe MR and a mobile echogenic density on the MV which was concerning for a vegetation vs tumor. He was started on broad-spectrum antibiotics due to suspicion of infective endocarditis(IE). A transesophageal echocardiogram (TEE) revealed a ruptured papillary muscle head mimicking a vegetation/tumor. The patient underwent MV replacement. Intraoperative findings demonstrated papillary muscle necrosis and rupture without evidence of valvular vegetation or tumor. Of note the patient did not improve despite the above efforts; echo done 2 days later showed EF 10-15%. The prognosis was explained to the family, and they transitioned the patient to hospice.
Conclusion / Discussion: Papillary muscle rupture is a very rare complication, known to occur in MI and IE. However, papillary muscle rupture leading to acute severe MR from cocaine toxicity is extremely rare. Cardiac catheterization and TEE ruled out MI and IE in our patient. Hence, he was thought to have developed cocaine-induced papillary muscle ischemia leading to its rupture. This was confirmed by intraoperative inspection of the papillary muscle and the valve apparatus (Pathologic examination of the resected papillary muscle showed atherosclerotic changes in small arteries and infarcted areas in different post infarct time phases along the ruptured edge). This case highlights the fact that mechanical complications typically associated with myocardial infarctions caused by coronary occlusions can also occur from a result of vasospastic and toxic processes as long as they cause significant ischemia. Prompt diagnosis and early surgical management is of utmost importance given the morbidity and mortality of the condition.
-
 and PDXI (MODY4) Variants in a Young Adult and Critical Therapeutic Implications by Shay-Kay Lambert-Johnson, Matthew Doan, and Megan Wesling")
Concurrent HNF1A (MODY3) and PDXI (MODY4) Variants in a Young Adult and Critical Therapeutic Implications
Shay-Kay Lambert-Johnson, Matthew Doan, and Megan Wesling
BACKGROUND: Monogenic diabetes accounts for approximately 1–5% of diabetes cases and is frequently misclassified. Maturity-onset diabetes of the young (MODY) includes 14 subtypes with distinct pathophysiology and therapeutic implications. Digenic MODY, caused by pathogenic variants in more than one MODY gene, occurs in well under 1% of cases and poses unique diagnostic and management challenges. We report the first known case of concurrent HNF1A (MODY3) and PDX1 (MODY4) mutations, highlighting important clinical and therapeutic considerations.
CASE PRESENTATION: A 19-year-old male with digenic MODY due to MODY3 (HNF1A) and MODY4 (PDX1) mutations presented for team-based adult outpatient diabetes management following transition from pediatric care. He had a BMI of 26.70 kg/m2 and reported instances of polydipsia, polyuria, and nocturia, but denied any visual changes, fatigue, dizziness, nausea, vomiting, or diarrhea. Genetic testing was performed at a tertiary hospital, establishing the dual mutation diagnosis. He was previously treated with basal-bolus insulin, but he reported poor compliance and therapy discontinuation due to access barriers. He was also not on insulin at the time of presentation. Initial laboratory evaluation demonstrated a hemoglobin A1c of 12.7%, SCr of 0.84, eGFR of >120, and a UACR of 4. Given uncertainty regarding beta-cell reserve in the setting of a concurrent PDX1 mutation, treatment was initiated with metformin (500 mg orally once daily) and low-dose basal–bolus insulin (insulin aspart 3 units subcutaneously three times daily with meals and insulin glargine 8 units subcutaneously once daily). At his one-month follow-up appointment, reported home glucose monitoring revealed a fasting glucose value of 110-120 mg/dL, pre-lunch values of 120-130 mg/dL, pre-dinner values of 160-170 mg/dL, and bedtime values of 130-140 mg/dL. With his stable glucose trends and patient preference for reduction in insulin burden, metformin increased to 500 mg orally twice daily and continued his low basal insulin.
DISCUSSION: This case represents the first reported instance of concurrent MODY3 and MODY4 mutations, illustrating how dual transcription factor defects can modify expected phenotypes and treatment responses. While MODY3 typically responds to sulfonylureas, the presence of a PDX1 mutation and marked hyperglycemia raised concern for limited beta-cell reserve, supporting early insulin initiation. Despite severe hyperglycemia, the patient achieved rapid improvement on low-dose insulin, suggesting preserved insulin sensitivity with impaired insulin production. This case adds to the limited literature on digenic MODY and underscores the importance of individualized, genotype-informed management to avoid misclassification and optimize outcomes.
-

Cor Triatriatum Sinistrum: An Underrecognized Indication for Anticoagulation
Boney Lapsiwala, Karthik Kasireddy, Tenna Mathew, and Babu Makkena
Background: Cor triatriatum (CTS) is a rare congenital heart defect in which a fibromuscular membrane divides the atrium into two chambers, disrupting normal blood flow and potentially leading to circulatory impairment. Accounting for 0.1% to 0.4% of congenital heart diseases, CTS presents variably depending on the degree of left atrial obstruction. Patients may report exertional dyspnea, orthopnea, or palpitations; severe cases can progress to heart failure, pulmonary hypertension, or thromboembolic events. We present the case of a young adult male who developed symptomatic heart failure and atrial fibrillation and was incidentally found to have CTS on imaging.
Case presentation: A 32-year-old male with a history of cocaine use presented with progressive dyspnea at rest and palpitations (NYHA IV). On admission, ECG showed atrial fibrillation (AF) with rapid ventricular response. Transthoracic echocardiography (TTE) demonstrated severe left ventricular systolic dysfunction (EF 15–20%), marked left atrial enlargement, and a fibromuscular membrane within the left atrium. Transesophageal echocardiography (TEE) showed two membrane fenestrations with a hemodynamically significant mean intra-atrial gradient of (~9 mmHg), dense spontaneous echo contrast within the proximal chamber, a small interatrial communication with left-to-right shunting, and a bicuspid aortic valve without significant stenosis or regurgitation (Group 3 Loeffler classification). Coronary CT angiography (CCTA) confirmed the diagnosis and excluded obstructive coronary artery disease. The patient was medically stabilized with diuresis, guideline-directed medical therapy for heart failure (HF), rate and rhythm control for atrial fibrillation, and anticoagulation with apixaban with symptomatic improvement. Definitive surgical or catheter-based membrane resection was recommended in accordance with adult congenital heart disease guidelines; however, due to financial and insurance constraints, the patient elected to defer invasive intervention and continue conservative management with close follow-up.
Lesson-Learned: CTS can present for the first time in adulthood with AF and acute decompensated HF, mimicking primary non-ischemic cardiomyopathy. The presence of large fenestrations does not exclude hemodynamically significant obstruction; physiologic assessment is essential. A fixed intra-atrial pressure gradient may increase left atrial pressure, post-capillary pulmonary hypertension, AF, and secondary ventricular dysfunction, highlighting both upstream-downstream pathophysiologic relationship. Multimodality imaging, including TTE, TEE, CCTA is essential to define membrane morphology, quantify obstruction, and identify associated congenital anomalies. Anticoagulation is a key component of management in adults with CTS and AF, even when traditional CHA₂DS₂-VASc scores are low.
Conclusion: CTS can present as cardiomyopathy in adults, requiring hemodynamic assessment and early anticoagulation.
-

Cost Effectiveness of Lifestyle Program for Diabetes Remission in the Era of GLP-1
Prasanthi Tondapu, Haasini Sunkavalli, Micaela C. Karlsen, Kara L. Staffier, Kathryn J. Pollard, and Surabhi NaIk
BACKGROUND: GLP-1 receptor agonists are popular for managing type 2 diabetes (T2D) and obesity but are costly and can result in side effects including weight rebound. Intensive therapeutic lifestyle change (ITLC) programs present an effective alternative, facilitating an HbA1C (A1C) less than 6.5% for 3 months without medication and long-term weight control.
CASE PRESENTATION: We present a 69-year-old Black man with T2D, hypertension, chronic kidney disease, obesity, and sleep apnea. In 2023, he was hospitalized with a blood glucose of 800 mg/dL and A1C 10.8% and discharged on insulin. And, with a BMI of 32 kg/m2 and weight of 238.6 pounds, he began treatment with semaglutide. Insulin was discontinued and the semaglutide dose was gradually increased to 2mg weekly. In one year, his A1C improved to 6.5% and weight decreased to 227 lbs. In 2024, he enrolled in an ITLC program for T2D remission based on the LEADR (Lifestyle Empowerment Approach for Diabetes Remission) curriculum, including shared medical appointments, diabetes and nutrition coaching, exercise sessions, psychological support, and continuous glucose monitoring (CGM).
14 weeks into the ITLC program, he discontinued semaglutide with an A1C of 5.7%. He maintained an A1C of 5.8% by program's end. His A1C fluctuated but stabilized at 5.9% one year later without medication, indicating remission. At the start of the program, his waist circumference (WC) was 42 inches, BMI 32 kg/m², and weight 220.3 lbs. After one year, his WC was 37 inches, BMI to 28.5 kg/m², and weighed 198.2 lbs. His first 14 weeks on semaglutide, he lost 10 lbs (-4.6%) and 16 lbs (-7.4%) total by the program's end. Overall, he lost 21 lbs (-10%), including 12 lbs (-5.6%) after stopping semaglutide. His body fat decreased from 59.8 lbs (27%) to 50 lbs (22%) and visceral fat area from 126.4 to 93.8. He discontinued antihypertensive medication, improved his sleep apnea, engaged in pickleball, and reported increased energy. Through the ITLC program, he achieved diabetes remission and continues to maintain it.
CONCLUSION:
This case demonstrates that comprehensive ITLC programs can promote sustained weight loss, improve metabolic parameters, enhance quality of life, reduce cardiovascular risk, deprescribe medication, and achieve diabetes remission. Similar programs could provide scalable, provider and payer-friendly models for T2D remission to decrease reliance on GLP-1RAs and lower long-term healthcare costs
-
 by Sienna Luk, Alvin Mathew, Darshan Bhatty, and Kamran Rizvi")
Devising a Protocol for MRI Clearance in Patients with Cardiac Implantable Electronic Devices (CIED)
Sienna Luk, Alvin Mathew, Darshan Bhatty, and Kamran Rizvi
Background: Magnetic Resonance Imaging (MRI) in patients with Cardiac Implantable Electronic Devices (CIEDs) remains a logistical challenge in many clinical settings. At Medical City Denton, the absence of a standardized institutional policy has led to significant inefficiencies, including prolonged hospital stays and increased healthcare costs. The primary objective of this project was to address these barriers by developing a streamlined, evidence-based protocol to improve care coordination and resource utilization for patients with CIEDs requiring diagnostic imaging.
Methods: Launched in 2026, this pilot initiative utilized a multi-stakeholder approach involving hospitalists, EPs, radiology staff, and device representatives. A core component of the intervention was the implementation of a new clinical algorithm designed to bypass the traditional EP consult for patients meeting specific safety criteria:
Device Status: Confirmed MRI-conditional device from Medtronic or Abbott. Lead Integrity: Chest X-ray (CXR) within the previous 5 months confirming no abandoned, retained, fractured, or epicardial leads.
Documentation: Verified patient consent and existing device documentation. The primary metrics for evaluating the pilot’s efficacy included hospital Length of Stay (LOS) and the "Time-to-Imaging" interval. Results: Already have established baseline year round data from 2025. Plan to implement new policy in February, 2026.
Conclusion: (Pending collecting data and result) Implementing a criteria-based algorithm for CIED-MRI clearance effectively reduces administrative delays without compromising patient safety. By delegating clearance for documented, stable Medtronic and Abbott systems to a standardized pathway, institutions can optimize specialist utilization and decrease the total cost of care. This pilot serves as a model for a planned division-wide rollout.
-

Don’t Blame The Heart When on Steroids: A Rare Case Of Glucocorticoid Dependant Childhood Asthma Causing Non-Ischemic Dilated Cardiomyopathy
Greeshma Molugu, Srinivasan Rajaganapathy, Machaiah Madhrira, and Karthik Anand
Background: Steroids are known to have various cardiac side effects, such as hypertension, left ventricular hypertrophy, myocardial infarction, and sudden cardiac death. They are also known to cause rare but potentially life-threatening cardiomyopathy. The mechanisms behind steroid-induced cardiomyopathy are multifactorial, potentially involving direct or indirect myocardial toxicity, such as tissue fibrosis, apoptosis, and alterations in cardiac remodeling pathways via the renin-angiotensin-aldosterone system. Cardiomyopathy is known to occur with anabolic steroid use, but the literature on glucocorticoid-induced cardiomyopathy is scant. We present a rare case of glucocorticoid-induced dilated cardiomyopathy(DCM) in a patient with a history of refractory asthma who was treated with oral prednisone for greater than 40 years.
Case Description: A 46-year-old male with a history of childhood asthma treated with oral prednisone since the age of eight months presented with worsening exertional dyspnea and volume overload. Transthoracic echocardiogram(TTE) was remarkable for dilated left ventricle(LV) with reduced LV ejection fraction(EF) of 25-30%, along with diffuse hypokinesis. Given the new onset of decompensated heart failure with reduced EF, the patient underwent cardiac catheterization, which ruled out ischemic cardiomyopathy. After an extensive negative workup (including endocrine, drug screen, and autoimmune panel), the patient was diagnosed to have glucocorticoid-induced non-ischemic DCM. The patient was advised to taper the current steroid dose and follow up with a pulmonologist for asthma management. The patient was started on guideline-directed medical therapy (GDMT) for DCM and discharged on a life vest. At the six-month follow-up, the patient remained asymptomatic, and his EF improved to 45%. Resolution of the patient's symptoms with discontinuation of steroids confirmed the diagnosis of steroid-induced DCM.
Discussion: Steroid cardiomyopathy due to the overuse of anabolic steroids containing testosterone has been well-reported in the literature, but DCM due to the overuse of glucocorticoids is extremely rare. This case highlights the rare presentation of reversible DCM due to the chronic use of glucocorticoids. The reversible nature of this condition underscores the need for vigilance regarding steroid-induced cardiomyopathy, emphasizing early diagnosis, cessation of steroid use, and initiation of GDMT for improved outcomes. With increasing amounts of chronic steroid use for various disorders and recreational use, it is important to add steroid-induced cardiomyopathy to our lists of differentials for newly diagnosed heart failure patients.
-

Double Trouble: A Rare Co-Existence of Hypertrophic Obstructive Cardiomyopathy and Anomalous Origin of the Right Coronary Artery
Greeshma Molugu, Srinivasan Rajaganapathy, Seline Haci, and Machaiah Madhrira
Introduction: Hypertrophic obstructive cardiomyopathy (HOCM) and anomalous origin of the right coronary artery (RCA) are well-known but rare congenital heart diseases that are recognized as independent leading causes of sudden cardiac death(SCD). The independent prevalence of both these conditions is less than 1%. The co-occurrence of these two conditions is seldom ever reported in the literature. We present an extremely rare case of HOCM and the anomalous origin of the RCA in the same individual.
Background: A 67-year-old male with no significant past medical history presented for chest pain and palpitations. EKG showed atrial fibrillation with rapid ventricular response. Troponin level remained negative throughout the admission. Transthoracic echocardiography(TTE) revealed an ejection fraction (EF) of 55-60%, asymmetric septal hypertrophy of 18.92mm, hypokinesis of the inferoseptal myocardium, left ventricular outflow tract(LVOT) obstruction with mean gradient of 145mmHg, increased LVOT velocity. Transesophageal echocardiography(TEE) was remarkable for eccentric posteriorly directed mitral regurgitation(MR), sigmoid septum, and evidence of LVOT obstruction. Coronary computed tomography angiography (CCTA) showed anomalous origin of the right coronary artery, arising from the sinotubular junction of the aorta distal to the left coronary sinus located slightly superior and anterior to the origin of left main coronary artery. Cardiac MRI was remarkable for asymmetric septal hypertrophic cardiomyopathy. Additionally, systolic anterior motion of the mitral valve leaflet suggesting obstructive component was noted on the cardiac MRI. The patient underwent cardiac catheterization, which showed evidence of hypertrophic obstructive cardiomyopathy(HOCM) with a left ventricular aortic gradient of 90mmHg. Coronary angiography showed anomalous takeoff of the right coronary artery(RCA) from the left coronary cusp. The patient underwent trans-aortic septal myectomy along with repair of the anomalous RCA(unroofing). Surgical pathology of the specimen was compatible with the diagnosis of HOCM. The patient was later discharged on oral anticoagulation and rate control therapy. The patient was found to be symptom-free at his three-month follow-up. He was educated on genetic testing and the importance of generational family screening.
Conclusion: HOCM is a well-known inherited cardiac disease with a prevalence of approximately 1 in 500 adults. Congenital coronary anomalies are rare, with a prevalence of 0.3% in necropsy and almost 1% in coronary angiographic series. The literature on the co-existence of these two entities is extremely scant. This case highlights the uniqueness of the co-occurrence of both these conditions. Studies have reported that both these conditions are independently associated with an increased risk of SCD. Hence, this case focuses on the awareness of potential co-occurrence of these two conditions, which is especially important for risk stratification for SCD. Early diagnosis of these lethal conditions can improve the prognosis and survival rate. It is also essential to educate the patient on the importance of genetic testing.
-

Drug-Induced Acute Interstitial Nephritis Presenting as Severe Acute Kidney Injury Requiring Temporary Hemodialysis
Nihar Raju, Rohit Nair, Vaishnavi Singh, and Veeranna Vibhuti
Background: Acute interstitial nephritis (AIN) is an important but often underrecognized cause of acute kidney injury (AKI), accounting for 2–5% of all kidney biopsies and up to 20% of biopsies performed for AKI. Drug-induced AIN is the most common etiology in developed countries, frequently associated with antibiotics, nonsteroidal anti-inflammatory drugs, and proton pump inhibitors. Classic hypersensitivity features are frequently absent, leading to delayed diagnosis and increased risk of dialysis dependence.
Case Presentation: A 74-year-old male with a history of prostate cancer, type 2 diabetes mellitus, and hypertension presented with progressive exertional dyspnea and was found to have severe AKI without prior chronic kidney disease. Admission laboratory evaluation revealed creatinine 5.51 mg/dL, thrombocytopenia, and hyponatremia. Imaging showed no evidence of obstructive uropathy. Urinalysis demonstrated significant pyuria with white blood cell casts and elevated urine sodium, suggesting intrinsic renal injury. Etiology of AKI was suspected to be volume overload. Despite supportive management and diuresis, renal function worsened with creatinine increasing to 7.0 mg/dL and declining urine output, necessitating initiation of intermittent hemodialysis. Subsequent urine studies revealed eosinophiluria. Detailed medication reconciliation identified recent exposure to amoxicillin-clavulanate prior to admission. High-dose intravenous corticosteroids were initiated, followed by an oral prednisone taper. Kidney biopsy later confirmed inflammatory interstitial infiltrates consistent with AIN. Renal function gradually improved, dialysis was discontinued, and creatinine returned near baseline by hospital day eight.
Lessons Learned: This case illustrates the broad differential diagnosis of AKI and emphasizes the importance of early consideration of drug-induced AIN, even in the absence of classic hypersensitivity findings. Thorough medication review, timely nephrology consultation, and appropriate diagnostic evaluation are critical. While a subset of patients with AIN require temporary dialysis, early recognition and prompt corticosteroid therapy can result in renal recovery and avoidance of permanent dialysis.
Conclusion: Drug-induced AIN is a reversible cause of severe AKI that requires a high index of suspicion. Early identification and treatment are essential to improve renal outcomes, particularly in older patients with recent antibiotic exposure.
-
 Medications in Patients Undergoing Total Hip Arthroplasty (THA): A Systematic Review and Meta-analysis by Tanner Haechten, Troy B. Puga, Vincent Dieu, McKenna W. Box, Kyle O'Connor, and John T. Riehl")
Effects of Glucagon-Like-Peptide-1 Receptor Agonists (GLP-1a) Medications in Patients Undergoing Total Hip Arthroplasty (THA): A Systematic Review and Meta-analysis
Tanner Haechten, Troy B. Puga, Vincent Dieu, McKenna W. Box, Kyle O'Connor, and John T. Riehl
Background Glucagon-Like-Peptide-1 Receptor Agonists (GLP-1a) medications have rapidly grown in popularity, however, their effects on the outcomes of Total Hip Arthroplasty (THA) remain largely unclear. The objective of this systematic review and meta-analysis is to evaluate the outcomes of patients undergoing THA and using a GLP-1a medication. Methods A search was conducted across six databases. The search used a combination of keywords and Medical Subject Heading (MeSH) terms. Titles and abstracts were screened for eligibility for inclusion criteria. Full texts were screened and included if they met eligibility criteria. Demographics and results of the studies were extracted from included articles. Meta-analysis was conducted.
Results In this systematic review and meta-analysis, 10 studies met final inclusion criteria, and nine studies met inclusion for meta-analysis. Patients using GLP-1a medications in the setting of THA to those not using GLP-1a medications found a statistically significant decrease in the odds of readmission (OR: 0.81 (95% CI: 0.70-0.93); P< 0.001), and no significant difference in the odds of surgical site infections (OR: 0.85 (95% CI: 0.60-1.20); P=0.36). At 90 days, there was no significant difference in prosthetic joint infections (OR: 1.19 (95% CI: 0.92-1.54); P=0.18), periprosthetic fractures (OR: 1.17 (95% CI: 0.82-1.68); P=0.40), and surgical or medical complications (OR: 0.84 (95% CI: 0.68-1.03); P=0.10) (Figures 4-6). At 2 years, there was no significant difference in periprosthetic fractures (OR: 0.99 (95% CI: 0.53-1.84); P=0.97) or prosthetic joint infections (OR: 0.98 (95% CI: 0.67-1.44); P=0.93).
Conclusion The findings of this study suggest that patients using GLP-1a medications while undergoing THA had reduced 90 day readmission rates, with equivalent rates of SSI, medical and surgical complications, PJI at 90 days and 2 years, and periprosthetic fracture 90 days and 2 years when compared with those not using GLP-1a medications. GLP-1a medications may be safely used in patients undergoing THA.
-
 in Total Joint Arthroplasty (TJA): A Systematic Review and Meta-analysis by Jenna Chrabolowski, Troy B. Puga, Abanoub Attalah, Kyle P. O'Connor, McKenna W. Box, Ashley Stovall, Michael Muncy, and John T. Riehl")
Efficacy and Outcomes of Oxidized Regenerated Cellulose (ORC) in Total Joint Arthroplasty (TJA): A Systematic Review and Meta-analysis
Jenna Chrabolowski, Troy B. Puga, Abanoub Attalah, Kyle P. O'Connor, McKenna W. Box, Ashley Stovall, Michael Muncy, and John T. Riehl
Introduction Intraoperative and postoperative blood loss is a major concern and challenge for surgeons in total joint arthroplasty (TJA). Patients with large blood loss can develop postoperative anemia and associated complications. Novel hemostatic agents, such as oxidized regenerated cellulose (ORC) have grown in popularity as intraoperative hemostatic adjuncts. The aim of this systematic review and meta-analysis is to evaluate the efficacy of ORC for intraoperative and postoperative blood loss.
Methods A search was conducted across MEDLINE/Pubmed, Cochrane, Google Scholar, Web of Science, and Embase databases. Titles and abstracts were screened for eligibility for inclusion criteria. Full texts were screened and included if they met eligibility criteria. Demographics and results of the studies were extracted from the articles that met inclusion criteria. Meta-analysis was conducted to evaluate outcomes.
Results Eleven studies met inclusion criteria. There were four Level 1 evidence studies, one Level 2 evidence study, five Level 3 evidence studies, and one Level 4 evidence study. One case report study did report a hypersensitivity reaction, however, the remaining studies showed no additional complications from the use of ORC. Five studies reported equivalent rates of blood transfusion, with one study finding that ORC led to lower rates of blood transfusions. Nine studies were included for meta-analysis. Total blood loss (Cohen’s d: -0.42, CI: -0.66- -0.19, p< 0.001) and intraoperative blood loss (Cohen’s d: -0.33, CI: -0.51- -0.14, p< 0.001) were significantly lower in the ORC cohort compared to using no ORC. The ORC cohort also had significantly lower hemoglobin drop on postoperative day 1, however, publication bias was present in association with this finding. There was no significant difference between the ORC cohort and the no ORC cohort for postoperative day 7 hemoglobin (Cohen’s d: 1.13, CI: -0.15- 2.42, p=0.08), postoperative day 1 C-Reactive Protein (CRP) (Cohen’s d: 0.09, CI: -0.10- 0.29, p=0.36), and postoperative day 7 CRP (Cohen’s d: 0.04, CI: -0.50- 0.58, p=0.88).
Conclusion ORC may help to reduce total blood loss and intraoperative blood loss in TJA, however, it does not appear to have sustained effects over the following week, nor does it appear to lower transfusion rates with the current available evidence. ORC has been shown to be safe, with CRP levels remaining constant postoperatively, and only one case report showing a self-limited hypersensitivity reaction (local rash). ORC may be a useful adjunct to help reduce blood loss for TJA, however, it is not currently clear if its usage leads to significant improvements in clinical outcomes.
-

Efficacy of Zuranolone in the Treatment of Postpartum Depression: An Evidence-Based Review
Shana-Kay Lambert-Johnson and Tasaduq Mir
BACKGROUND: Postpartum depression (PPD) is a common and potentially severe condition frequently managed in primary care, where delayed treatment adversely affects maternal and infant outcomes. Neuroactive steroid therapies targeting γ-aminobutyric acid type A receptors represent a novel therapeutic class. Brexanolone, the first FDA-approved treatment for PPD, required prolonged inpatient administration and was withdrawn from the U.S. market in 2025. Zuranolone is currently the only FDA-approved medication specifically indicated for PPD, offering a short-course oral treatment suitable for outpatient use. This review evaluated the efficacy of zuranolone and its applicability in primary care practice.
METHODS: This evidence-based review was conducted in accordance with PRISMA 2020 guidelines. A search was performed using PubMed, from 2021 to January 2026. Search terms “zuranolone,” “postpartum depression”. Eligible studies were randomized, double-blind, placebo-controlled trials enrolling adults with PPD, baseline 17-item Hamilton Depression Rating Scale (HAMD-17) scores. Two phase 3 trials (ROBIN and SKYLARK; n=349) were included. These trials enrolled women aged 18-45 years, ≤6 months postpartum, with severe postpartum depression (HAMD-17 score ≥26) and onset in the third trimester or within 4 weeks postpartum. Participants were randomized 1:1 to receive zuranolone (30 mg in ROBIN, n=153; 50 mg in SKYLARK, n=196) or placebo.
RESULTS: For the primary outcome, both trials demonstrated statistically significant superiority over placebo at day 15, with mean HAMD-17 score reductions favoring zuranolone by −4.2 points in ROBIN (95% CI −6.9 to −1.5; P=0.003) and −4.0 points in SKYLARK (95% CI −6.3 to −1.7; P0.001). Antidepressant effects emerged by day 3 and were sustained through day 45. For secondary outcomes, response rates at day 15 were 72% with zuranolone versus 48% with placebo in ROBIN, and remission rates were 45% versus 23% (number needed to treat of 5 for both). Zuranolone also improved anxiety symptoms (HAM-A) and maternal functioning (Barkin Index). Adverse events were predominantly CNS-related, and were generally mild to moderate.
CONCLUSION: Zuranolone offers rapidly acting, short-course oral treatment for severe postpartum depression and represents a meaningful therapeutic advance for primary care. Its use, however, is limited by high cost, variable insurance coverage, restriction to severe PPD populations, controlled substance classification, limited long-term data, and the absence of head-to-head comparisons with selective serotonin reuptake inhibitors or psychotherapy. Further research is needed to clarify comparative effectiveness, cost-effectiveness, patient selection, and long-term outcomes.
-

Esophageal Squamous Cell Carcinoma Incidentally Detected on Barium Swallow: A Case Report
Muhammad Rubeel Akram, Aditya Rao, and Muhammad T. Siddique
Background: Esophageal cancer is an aggressive malignancy with a poor prognosis, and has high rates of recurrence despite curative-intent therapy. While endoscopy with biopsy remains the gold standard for diagnosis, non-diagnostic imaging studies are performed when evaluating for dysphagia, and may bring to light underlying pathology, warranting further workup. Surgical resection following neoadjuvant chemoradiation is often performed, but postoperative complications and disease recurrence are important concerns. This case highlights the crucial role of early detection via imaging and the clinical burden associated with esophageal squamous cell carcinoma.
Case Presentation: A 76-year-old female presented with dysphagia and underwent a barium esophagogram, which revealed an abnormality that led to further evaluation. Subsequent diagnostic workup led to the diagnosis of esophageal squamous cell carcinoma. She was treated with neoadjuvant chemoradiation followed by McKeown esophagectomy with cervical anastomosis. The postoperative course was complicated by a small, contained anastomotic leak distal to the anastomotic site, which was successfully managed with endoscopic vacuum therapy and conservative measures. The patient later developed recurrent squamous cell carcinoma in situ and required additional treatment, but unfortunately passed away shortly after.
Conclusion: This case underscores the importance of thoroughly evaluating patients presenting with relatively benign-appearing symptoms that may be indicative of underlying disease, and demonstrates how non-diagnostic imaging can aid in the diagnosis of malignancy. It also highlights the clinical impact of the type of esophagectomy performed, as cervical anastomosis has been associated with higher rates of anastomotic leak as compared to intrathoracic anastomosis. Furthermore, this case illustrates that the recurrence of squamous cell carcinoma may occur despite neoadjuvant chemoradiation and curative-intent surgery, emphasizing the limitations of current treatment options and the need for individualized decision-making that weighs both long-term health outcomes and quality of life.
Lessons Learned: This case reinforces the diagnostic value of early imaging in the evaluation of dysphagia and highlights the impact of postoperative complications on patient outcomes. This case also emphasizes the risk of recurrence in esophageal cancer despite a comprehensive treatment plan. Further research should investigate strategies to reduce adverse postoperative outcomes and improve long-term quality of life.
-

Evaluating the Alt-70 Model for Cellulitis Management in the Emergency Department
Marshall Hall, Paige Loux, Henry Lim, Jeffrey Durbin, Garrett Furth, Olivia Gruver, Christina Guo, Dustin Wilkes, Michael Carletti, and Stephen E. Weis
Background: Cellulitis is a common skin infection that classically presents with unilateral lower extremity erythema, swelling, and pain. The diagnosis is made clinically. Many conditions may mimic cellulitis that are collectively referred to as “pseudocellulitis.” These include stasis dermatitis, deep vein thrombosis, atopic dermatitis, psoriasis, and gout. The Alt-70 model is a validated clinical prediction tool for differentiating cellulitis from pseudocellulitis. It is unclear if it is utilized or if it has changed clinical practice in the emergency department setting.
Methods: This was a retrospective chart review study utilizing the HCA Healthcare Data Warehouse. The Alt-70 model was applied using electronic medical record data to characterize patients as having cellulitis or pseudocellulitis. The study included persons, ages 18-89, who were admitted to a North Texas division HCA hospital from the emergency department between January 2022 and December 2024 with a diagnosis of lower extremity cellulitis or lower extremity venous disorder.
Results: The final sample included 3,138 patients with a mean age of 54.9 years. The sample was 39% female. 254 (8.1%) patients had a diagnosis of a lower extremity venous disorder. 567 (18.07%) of patients had an ALT-70 score of 0-2, 1,560 (49.71%) patients had a score of 3-4, and 1,011 (32.22%) had a score greater than 4. The mean Alt-70 score was 3.59. There was no significant difference between Alt-70 score groups (“treat” vs “reassess” and “consultation” vs “reassess”) and prescription of inpatient antibiotics (p=0.96, p=0.26). There was no significant difference between Alt-70 score groups and hospital length of stay (p=0.60, p=0.06).
Conclusion: This study found no significant difference between the Alt-70 groups and antibiotic administration or hospital length of stay. These data suggest an overdiagnosis of cellulitis and an overuse of antibiotics. This study aligns with previous research indicating an overuse of medical resources, which may contribute to antibiotic resistance, nosocomial infections, hospital admissions, and other treatment-related adverse events. Utilization of the Alt-70 model with forced functions in electronic health systems, as well as education amongst hospital teams, may allow for better utilization of these diagnostic tools. Large prospective studies implementing this tool should be performed to understand its impact on the diagnosis and treatment of cellulitis and its imitators.
-

Excision Followed by Standing Cone Deformity Repair is Tissue Conservative
Henry Lim, Christian Scheufele, Marshall Hall, Stephen Weis, and Dustin Wilkes
Introduction Elliptical excisions are the most common method to treat benign and malignant tumors in dermatologic surgery. This standardized design is traditionally 3 to 4.5 times longer than the excisional width to prevent unsightly protrusions of skin after primary closure, known as “standing cone,” “Burow’s triangles” or “dog ear” deformities. This results in a scar significantly longer than the original tumor that may be less easily concealed.
Objective To compare the final repair length of a tissue conservative method to remove skin tumors and close resultant defects against predicted repair length of traditional elliptical excision.
Methods Eighteen cases are presented and retrospectively studied. In these cases, circular excision or Mohs micrographic surgery (MMS) was performed for cutaneous malignancy. After wide undermining and re-evaluation of skin tension lines, a subcuticular suture was placed along the center of the defect parallel to the tension vectors. Standing cone deformities were excised in a standardized fashion so that the final sutured wound would lay flat and a final length was measured. A predicted final length was also estimated using a 3 to 1 ratio of the excision diameter. The sutured repair length was compared to the predicted repair length. Results Surgical sites of the 18 cases consisted of 10 face, 4 upper extremity, 1 lower extremity, and 3 neck. There were 16 repairs after MMS and 2 repairs after circular excision. Malignancies treated included 9 basal cell carcinomas, and 9 squamous cell carcinomas. Post-operative defect sizes ranged from 1.2 cm to 4.2 cm. 18 out of 18 sutured repairs were shorter than the predicted repair length. Standing cone repair resulted in an average 25.96% reduction in predicted repair length.
Conclusion Circular excision of lesions followed by standing cone repair is tissue conservative and complimentary to principles of MMS. This technique should also be highly considered over standard elliptical excision in dermatologic surgery scenarios to improve cosmetic outcomes. Furthermore, future studies should evaluate the effects of tissue dynamics and other clinically relevant geometric measures to optimize the traditional elliptical excision and closure technique.
-

Extra-Intestinal Clostridioides difficile Abscess in a Small Bowel GIST: A Rare Tumor-Associated Complication
Nicholas Gerden, Pradip Gautam, Asad Rehman, and Long Hoang
Extra-intestinal infections caused by Clostridioides difficile are exceedingly rare and typically occur in settings that disrupt the gastrointestinal barrier, including recent gastrointestinal surgery, bowel perforation or microperforation, and severe colonic disease.
We present the case of a 75-year-old man with abdominal pain and hemoperitoneum in the setting of a suspected small bowel leak secondary to an intestinal mass. Computed tomography angiography revealed an 11.0 × 9.6 cm pelvic fluid collection, prompting exploratory laparotomy with drainage of a pelvic abscess and evacuation of hemoperitoneum. Intraoperatively, a small bowel perforation caused by a 4.4 cm gastrointestinal stromal tumor (GIST) was identified. Operative anaerobic abscess cultures were monomicrobial, unexpectedly isolating Clostridioides difficile despite the absence of diarrhea or evidence of colitis on imaging. Surgical pathology confirmed a low-grade GIST with negative resection margins. Extra-intestinal C. difficile infection represents a rare but serious pathology, accounting for only a small fraction of reported C. difficile infection cases, with no published treatment guidelines. To our knowledge, extra-intestinal C. difficile abscess formation associated with small bowel GIST has rarely been reported, highlighting an unusual infectious complication of tumor-related bowel pathology.
This case underscores the importance of considering extra-intestinal C. difficile as a potential pathogen in intra-abdominal infections among patients with gastrointestinal malignancy. Early recognition may facilitate timely diagnosis, appropriate antimicrobial therapy, and improved outcomes.
-

Gastroduodenal Artery Coil Erosion Causing Pyloric Obstruction and Upper GI Bleeding
Corey Newman, Mahad Rehman, Cody Beltran, and Michael Carrick
Background Trans-arterial embolization (TAE) of the gastroduodenal artery (GDA) is a well-established and effective treatment for peptic ulcer bleeding and visceral pseudoaneurysms. Although generally safe, delayed migration or erosion of embolization coils into the gastrointestinal lumen is a rare but recognized complication that may occur months to years after the procedure. Proposed mechanisms include ischemic mucosal injury, mechanical pressure from the coil mass, and chronic inflammation. Clinical manifestations vary widely, ranging from occult bleeding and ulceration to perforation or gastric-outlet obstruction. Only a limited number of cases describing GDA coil erosion presenting with both bleeding and obstruction have been reported.
Case Presentation A 34-year-old man presented after a 20-foot fall. Initial trauma evaluation revealed no acute injuries; however, laboratory studies demonstrated profound anemia with a hemoglobin level of 3 g/dL. Following blood transfusion, upper endoscopy was performed and revealed active upper gastrointestinal bleeding with pyloric obstruction caused by a bundle of metallic wires. Review of prior imaging confirmed a history of remote GDA embolization, consistent with the endoscopic findings. The patient underwent exploratory laparotomy, which demonstrated erosion of embolization coils through the posterior gastric wall into the pyloric channel with an associated ulcer. The coils were surgically removed, and pyloroplasty with Graham patch repair was performed. His postoperative course was initially uncomplicated, and he was discharged on postoperative day seven. Two days after discharge, the patient was readmitted with nausea and vomiting. Cross-sectional imaging revealed a contained duodenal perforation and postoperative edema without evidence of an anastomotic leak. He was managed conservatively with bowel rest, nasogastric decompression, and intravenous antibiotics, resulting in full clinical recovery.
Lessons Learned
- Coil erosion is a rare but serious delayed complication of gastroduodenal artery embolization.
- Prior embolization should raise suspicion for coil migration or erosion in patients presenting with unexplained anemia, hematemesis, or gastric-outlet obstruction.
- Endoscopy and computed tomography are complementary diagnostic modalities, allowing visualization of intraluminal metallic foreign bodies and associated mucosal injury.
- Definitive management often requires surgical coil extraction and repair when endoscopic retrieval is not feasible or bleeding persists.
- Multidisciplinary collaboration among gastroenterology, interventional radiology, and surgery is critical for timely diagnosis and optimal patient outcomes.
Conclusion This case highlights a rare delayed complication of GDA embolization presenting with profound anemia and gastric-outlet obstruction years after the initial procedure. Awareness of coil erosion as a potential etiology is essential, particularly in patients with prior embolization and atypical presentations. Prompt recognition using combined endoscopic and imaging approaches, followed by definitive surgical management, can lead to favorable outcomes despite the severity of presentation.
-

Gastroparesis as Initial Feature of Neuromyelitis Optica Spectrum Disorder
Jasmine M. Silva, Jorim J. Parmar, Shivani Gandhi, and Sreevani Gudiseva
-

Handheld Magnet Screening of External Fixator Components: A Laboratory Assessment of Gross Ferromagnetism Relevant to MRI Safety
Troy B. Puga, McKenna W. Box, Lyn D. Ward, and John T. Riehl
Introduction Much controversy remains regarding the ability of patients with an external fixator in place to undergo Magnetic Resonance Imaging (MRI). The main concern for radiology departments is that the external fixator system components can lead to adverse events due to interactions of the external fixator and the magnet of the MRI. However, there is no clear evidence to support these claims or theories in the current literature. Yet, MRI’s are denied daily across the country for patients having an external fixator in place. Numerous patients with an external fixator would likely benefit from an MRI to prevent delayed care, such as patients with traumatic spine injuries, traumatic brain injuries, or patients with multiligamentous extremity injuries. In order to determine if there are magnetic properties of external fixators, this study aims to use a testing magnet to see if there are any magnetic interactions between the external fixators and the magnet.
Methods A 1000 gauss handheld test magnet was obtained. A #10 scalpel blade, Adson forceps, and a needle driver were used as control test items. The Synthes large external fixation system, Synthes small external fixation system, Stryker Hoffmann 3 external fixation system, Smith & Nephew MAVERICK external fixation system, the Arthrex ArthroFX external fixation system were tested. The bars, bar to pin connectors, Schanz screws and rod to rod connectors were tested for each external fixation system. The Synthes small external fixation system does not have a bar to pin connector, and this was not tested for this system. For each item, the magnet was tested at the following three locations: 1cm away from the object, 0.5cm away from the object, and in direct contact with the object. A positive result of magnetism was an object being attracted to the magnet with direct contact or movement, and a negative result being no attraction. Results were recorded for the objects.
Results All three control items exhibited positive magnetism at 1cm of distance, 0.5cm of distance, and direct contact. All of the external fixator components exhibited no signs of magnetism and had negative magnetism testing at 1cm of distance, 0.5cm of distance, and direct contact. All of the following components of the external fixator were negative for magnetism, including: the bars, bar to pin connectors, the rod to rod connectors, or Schanz screws.
Conclusion In this magnetism testing of external fixator components, all of the external fixator components demonstrated negative testing for magnetism. The external fixator components do not appear to have any magnetic properties or attraction. This research further supports the safety of patients obtaining an MRI with an external fixator in place
-

Hemoptysis and Shock from a Proximal Bronchial Artery Aneurysm Successfully Treated with Endovascular Embolization
Gautham Raghuthaman, Charmi Mehta, and Tamer Hudali
Background: Bronchial artery aneurysm (BAA) is a rare vascular abnormality and an uncommon cause of hemoptysis. Although many BAAs are asymptomatic, rupture can result in life-threatening hemorrhage and shock. Proximal BAAs arising near the bronchial artery origin are particularly rare and may be underrecognized due to nonspecific clinical and radiographic findings.
Case Presentation: Patient is a 49-year-old male with a history of pituitary tumor resection complicated by secondary adrenal insufficiency and hypothyroidism presented with three days of cough, fatigue, and hemoptysis. He was hypotensive and hypoxic on arrival and required vasopressor support with stress-dose corticosteroids. Computed tomography angiography (CTA) of the chest showed diffuse ground-glass opacities, hypertrophied right bronchial arteries, and a 14-mm proximal right bronchial artery aneurysm near its origin. Interventional radiology was consulted and patient stabilized after transcatheter bronchial artery coil embolization.
Lessons Learned: BAAs are infrequently encountered and often misdiagnosed due to overlapping presentations with pulmonary infection, malignancy, or pulmonary embolism. Importantly, the risk of rupture is independent of aneurysm size, underscoring the need for prompt recognition and intervention once identified. Multiphasic CTA is critical for diagnosis, as it allows precise localization, characterization of arterial anatomy, and procedural planning. Endovascular embolization represents a safe and effective treatment modality, even in patients presenting with hemodynamic compromise.
Conclusion: This case highlights proximal bronchial artery aneurysm as a rare but critical cause of hemoptysis and hemodynamic instability. In patients with hemoptysis and unexplained shock, particularly when imaging suggests hilar pathology, vascular etiologies should be considered. Early CTA and endovascular management can be lifesaving.
-

Impact of a Resident-Created Family Medicine Clerkship Guide on Medical Student Preparedness
Shana-Kay Lambert-Johnson, Tasaduq Mir, and Fredricka Barr
BACKGROUND: Third-year medical students enter the family medicine clerkship with strong foundations in the basic medical sciences. However, they can feel underprepared to meet the demands of outpatient care, including navigating clinic workflows, documenting efficiently, and leading patient-centered visits. This transition-to-clerkship learning curve may contribute to stress during a critical phase of clinical development. Structured educational support during this transition has the potential to enhance learner confidence, promote meaningful learning, and foster positive engagement with family medicine. Through resident-led quality improvement, this project aimed to improve medical student preparedness and confidence for the family medicine clerkship using a resident-created intervention.
METHODS: A prospective pre-post quality improvement initiative was conducted during a third-year medical student family medicine clerkship at an outpatient site. Guided by a learner needs assessment, residents developed a Family Medicine Clerkship Guide addressing clinic workflow, pre-charting strategies, patient presentation frameworks, documentation guidance, rotation expectations, and shelf exam preparation. Students completed anonymous pre- and post-clerkship surveys assessing preparedness (5-point Likert scale), anticipated challenges, satisfaction, and perceived applicability. Preparedness outcomes were compared descriptively, and effect size (Cohen’s d) was calculated to assess educational impact. This project was deemed quality improvement and exempt from institutional review board review.
RESULTS: Pre-clerkship surveys were completed by 31 students, and post-clerkship surveys by 21. Baseline preparedness was low to moderate (mean 3.13), with 42% of students reporting being mostly or fully prepared. Following implementation of the clerkship guide, preparedness improved substantially (post mean 4.10; Cohen’s d ≈ 0.9), with 81% reporting being mostly or fully prepared and no students reporting being slightly or not prepared. Students identified pre-charting workflows, patient presentation frameworks, documentation guidance, and shelf exam preparation as the most helpful components. Learner satisfaction was high: 91% agreed or strongly agreed the guide provided tools applicable to outpatient clerkship activities, 96% felt it would positively impact their rotation, and 91% were likely or very likely to recommend it to peers. Few clarity concerns were identified, with one suggestion to incorporate visual aids for electronic health record templates.
CONCLUSION: A resident-created family medicine clerkship guide meaningfully improved medical student preparedness and confidence for outpatient clerkship care, addressing a common transition gap in undergraduate medical education. This scalable, low-cost intervention demonstrates the value of resident-led quality improvement in enhancing ambulatory learning environments while simultaneously supporting resident-as-teacher development. Similar onboarding tools may be adaptable across outpatient clerkships to improve learner readiness and experience.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
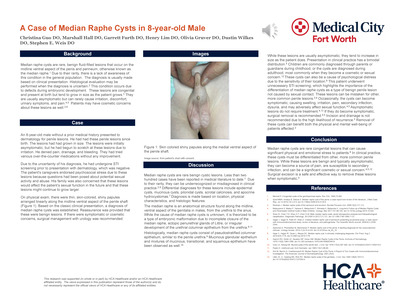{kind=link}
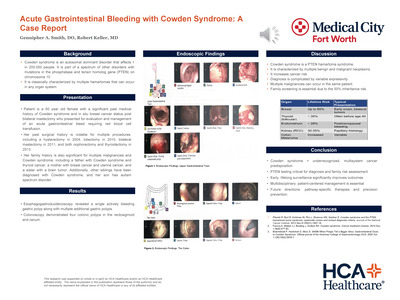{kind=link}
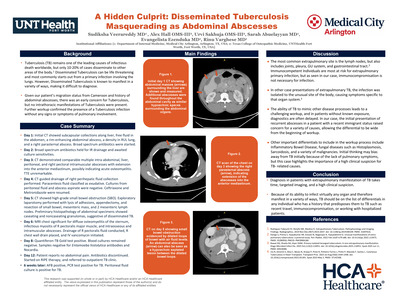{kind=link}
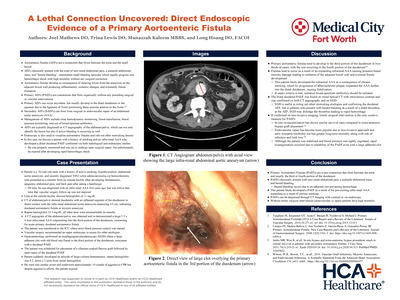{kind=link}
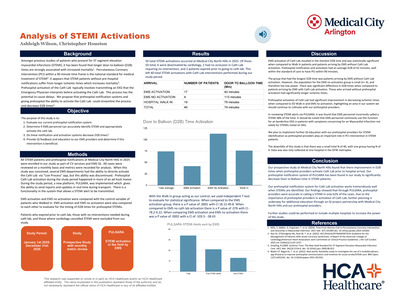{kind=link}
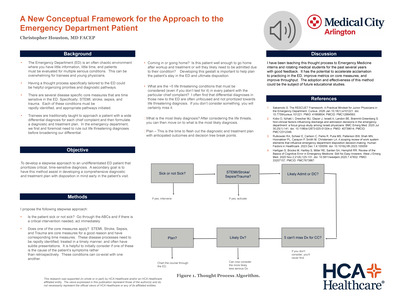{kind=link}
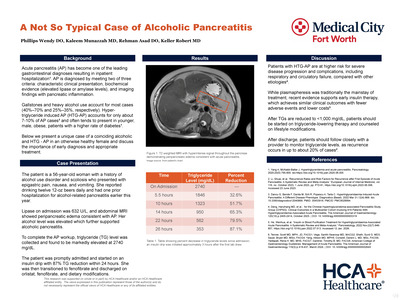{kind=link}
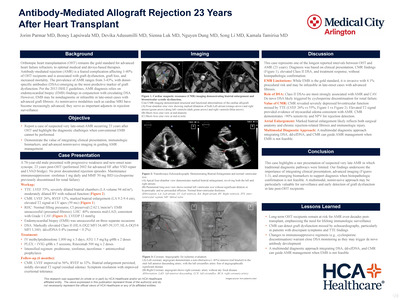{kind=link}
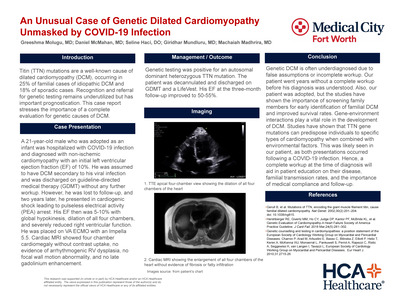{kind=link}
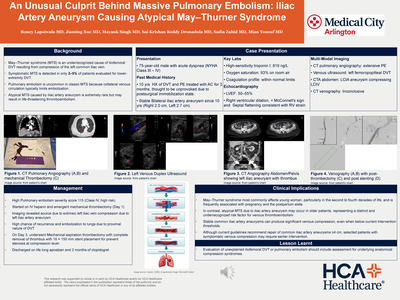{kind=link}
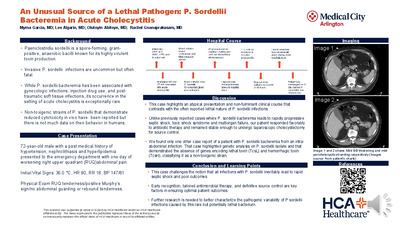{kind=link}
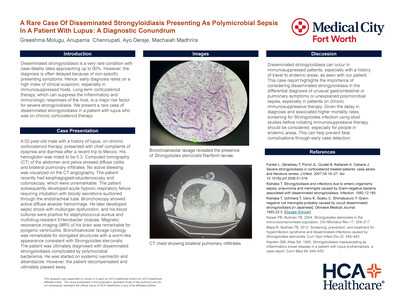{kind=link}
{kind=link}
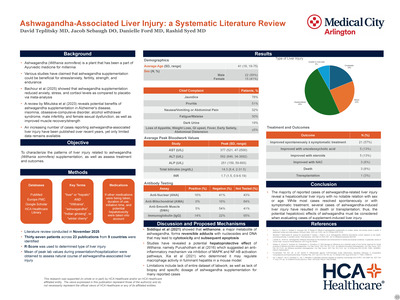{kind=link}
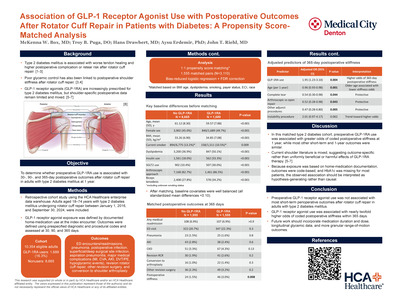{kind=link}
{kind=link}
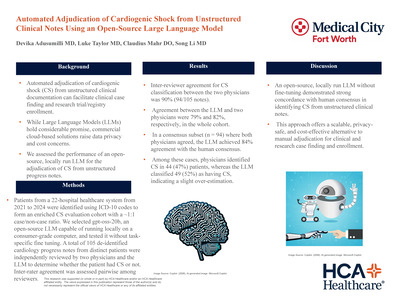{kind=link}
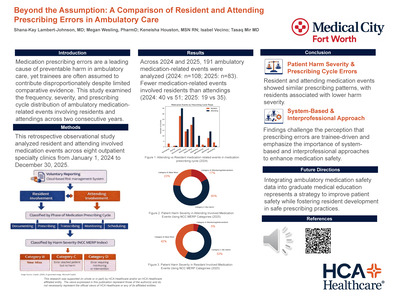{kind=link}
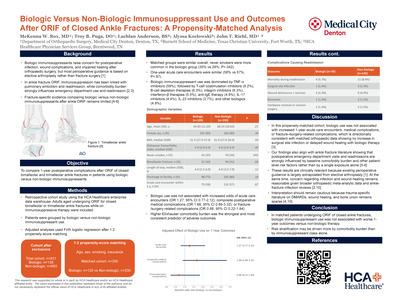{kind=link}
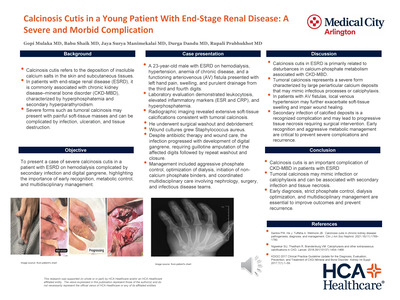{kind=link}
{kind=link}
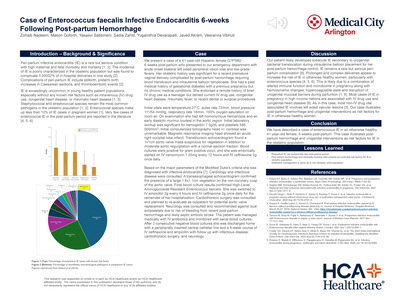{kind=link}
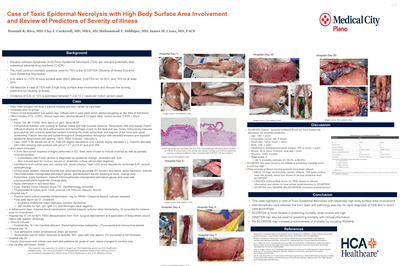{kind=link}
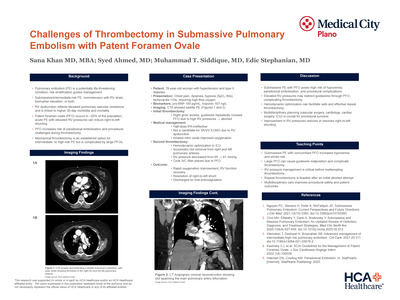{kind=link}
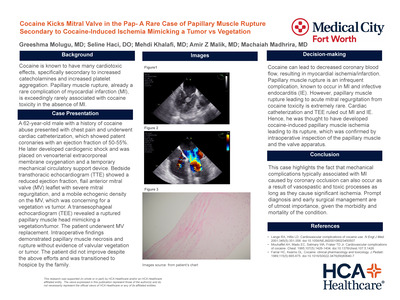{kind=link}
{kind=link}
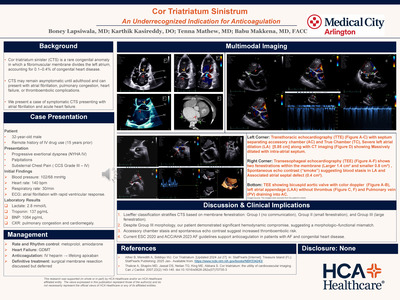{kind=link}
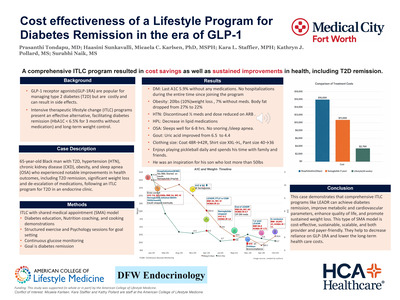{kind=link}
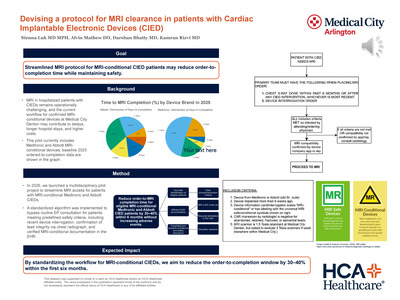{kind=link}
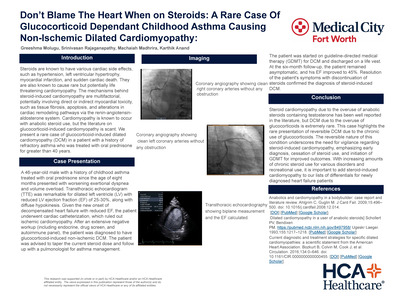{kind=link}
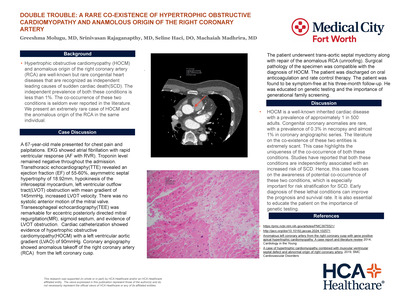{kind=link}
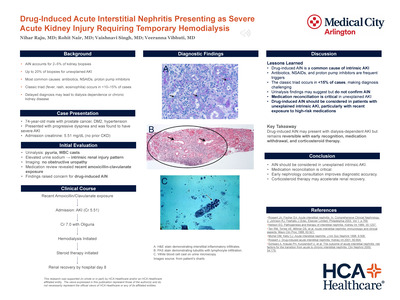{kind=link}
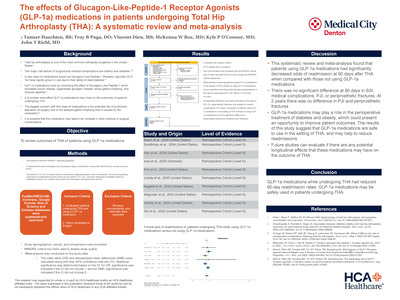{kind=link}
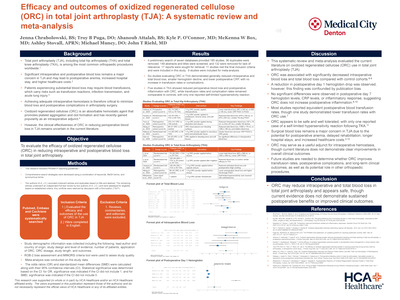{kind=link}
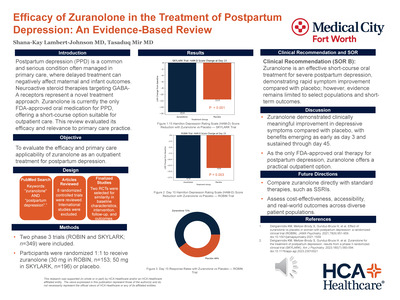{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
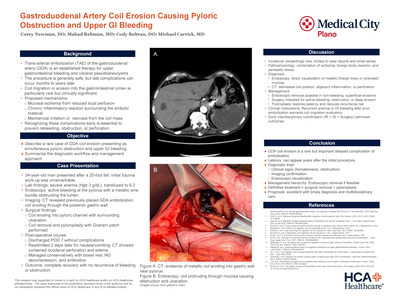{kind=link}
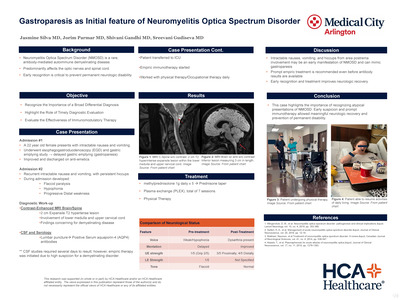{kind=link}
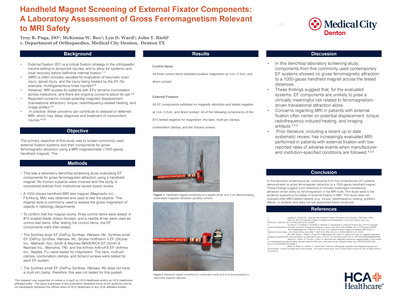{kind=link}
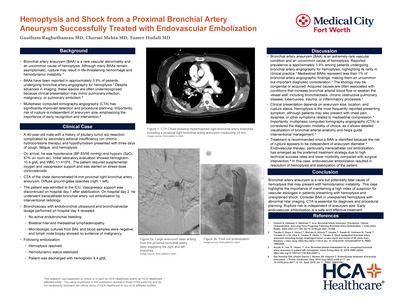{kind=link}
{kind=link}
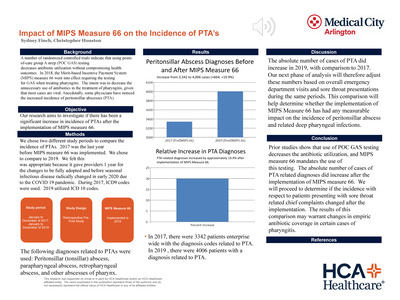{kind=link}
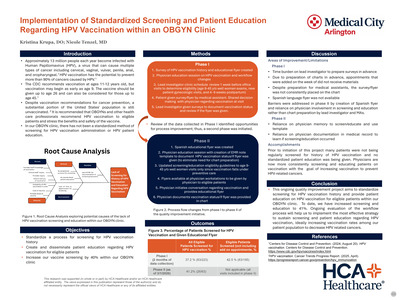{kind=link}
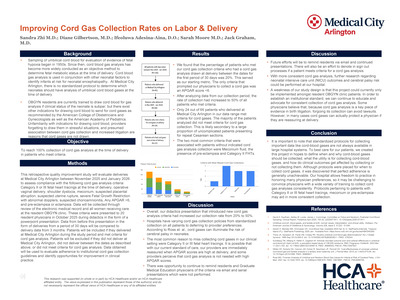{kind=link}
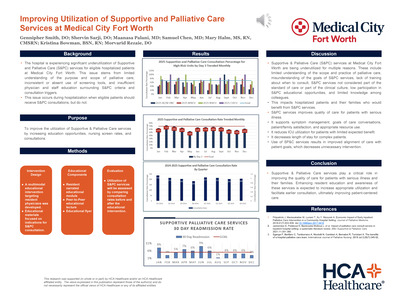{kind=link}
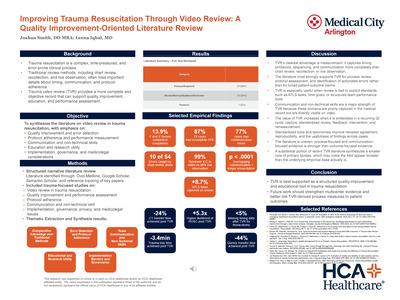{kind=link}
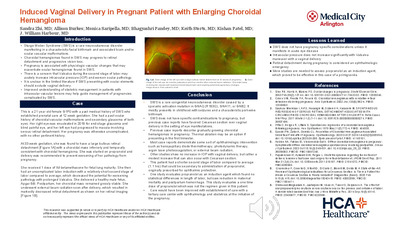{kind=link}
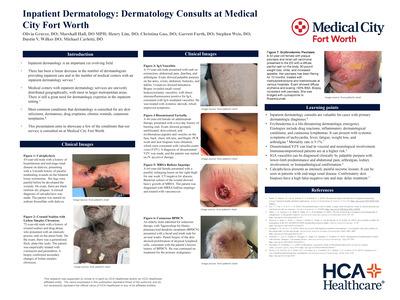{kind=link}
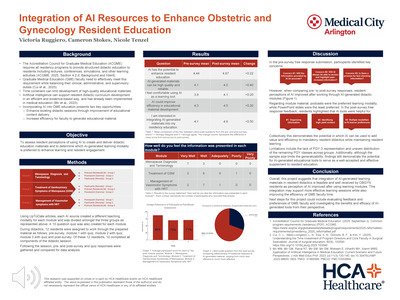{kind=link}
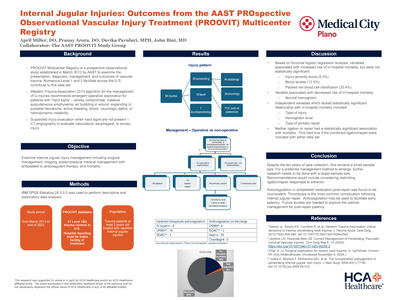{kind=link}
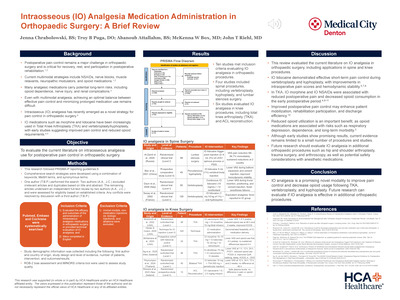{kind=link}
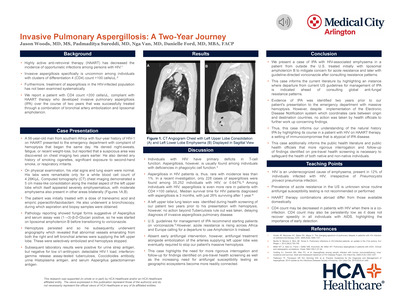{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
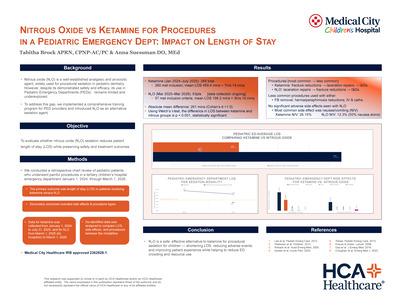{kind=link}
{kind=link}
{kind=link}
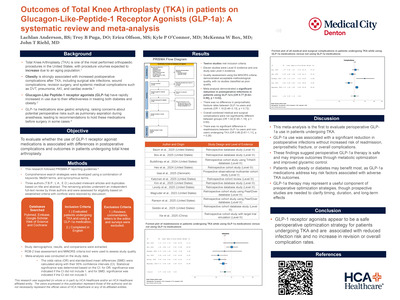{kind=link}
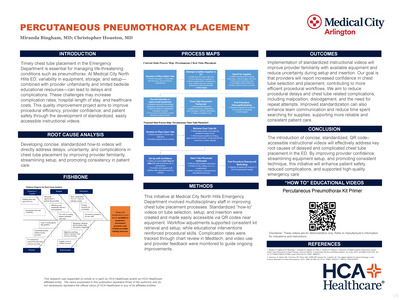{kind=link}
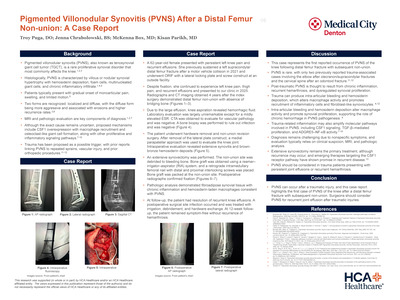{kind=link}
{kind=link}
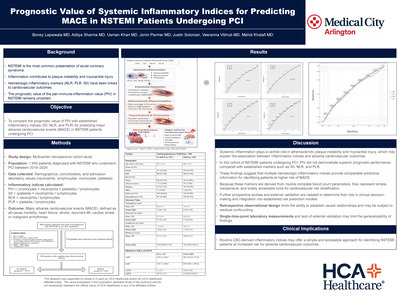{kind=link}
{kind=link}
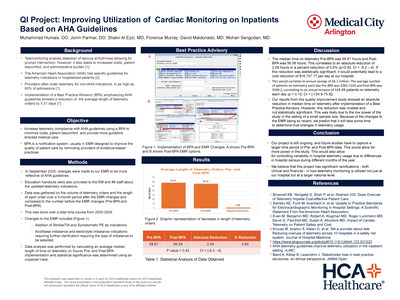{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
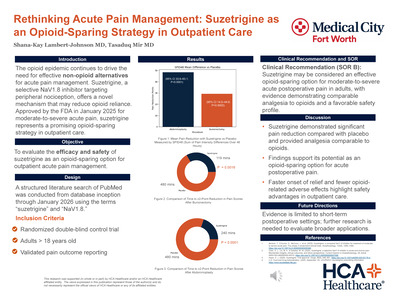{kind=link}
{kind=link}
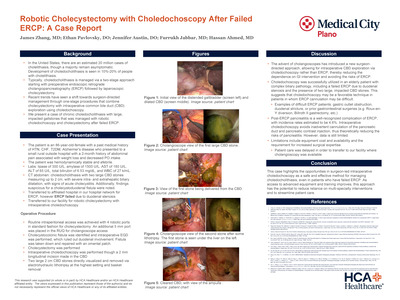{kind=link}
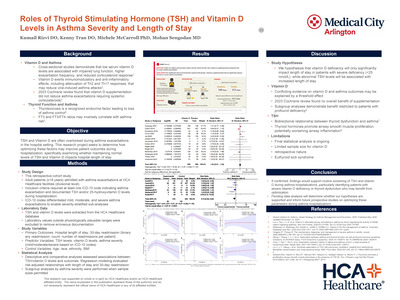{kind=link}
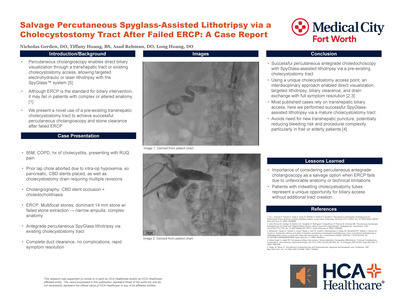{kind=link}
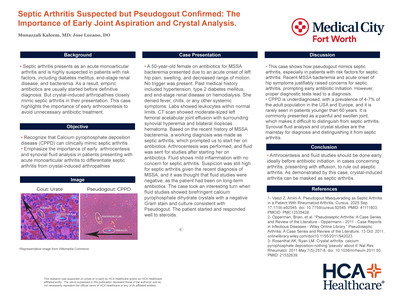{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
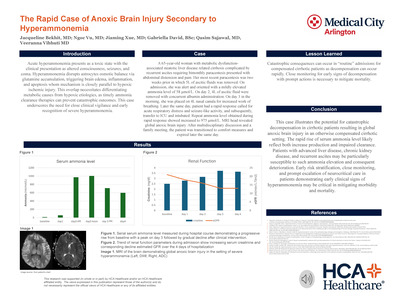{kind=link}
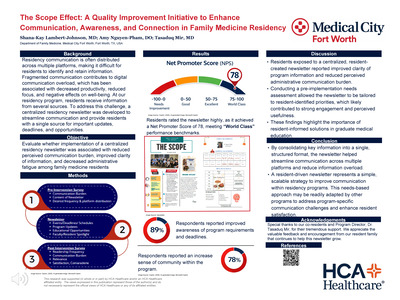{kind=link}
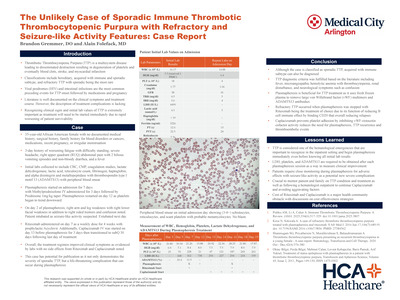{kind=link}
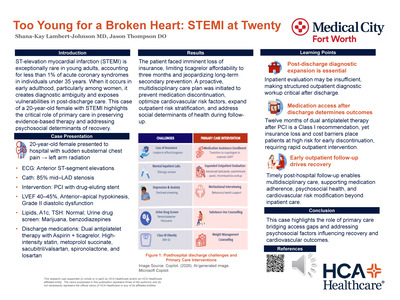{kind=link}
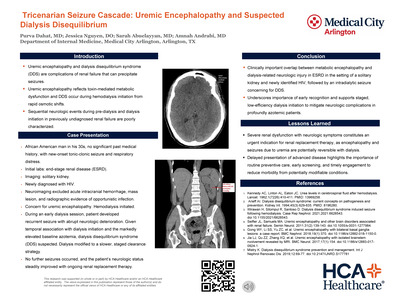{kind=link}
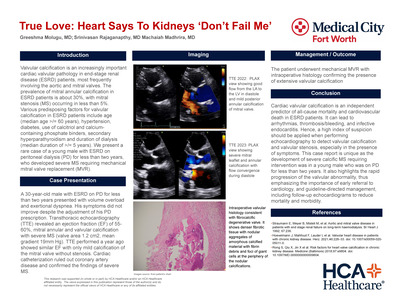{kind=link}
{kind=link}
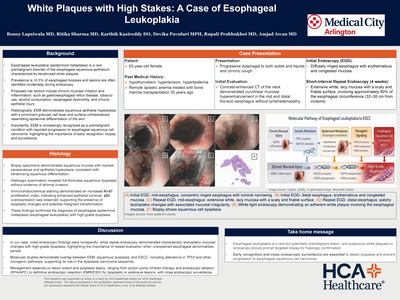{kind=link}